I really think this Doctor is correct?
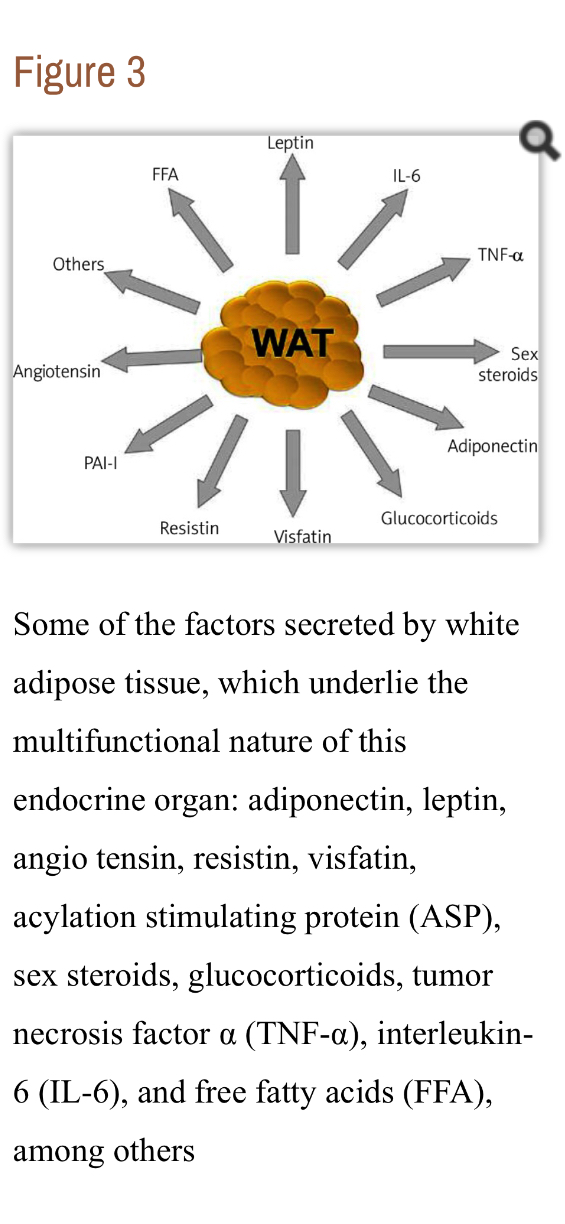
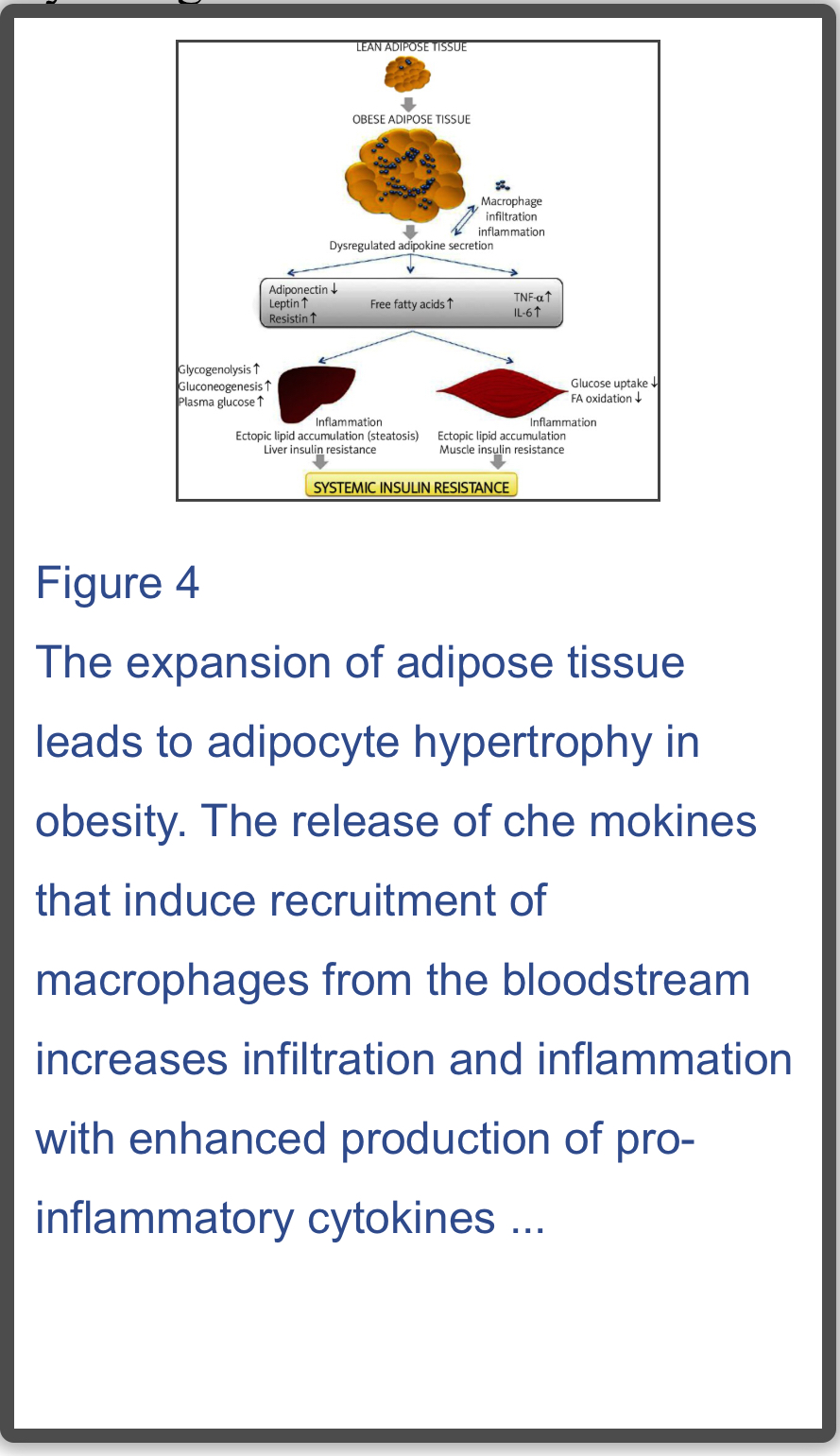
Keto is going to bump estrogen levels up even if your post-menopausal (see that a lot on this forum) and your ovaries are intact (hysterectomy?) they will start working again (spotting), so that’s where the configuration ratio starts?
If there is a hysterectomy and no weight loss on keto then there may still need to be a hormonal configuration ratio?
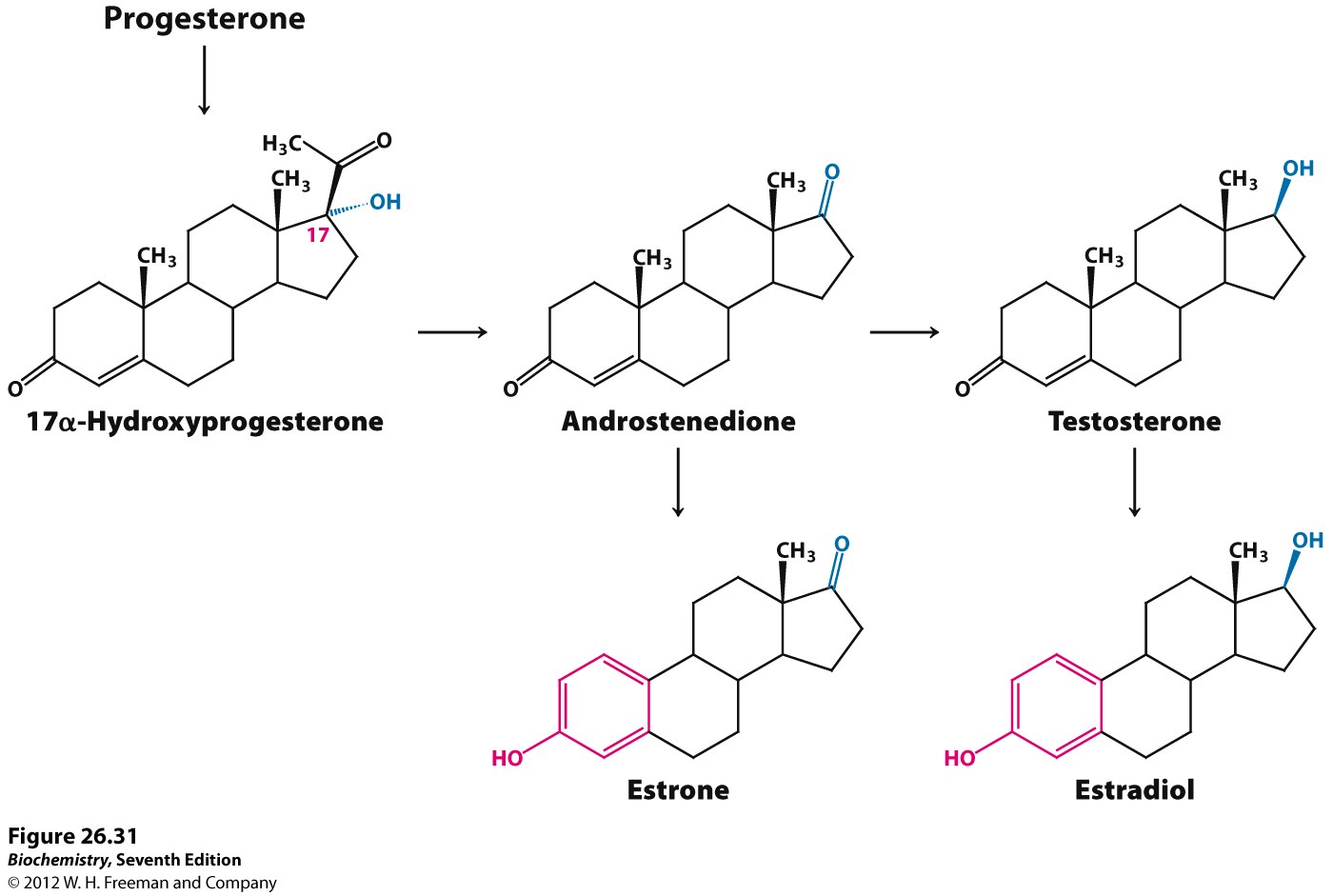
Understanding Your Progesterone to Estrogen Ratio - Dr. Houston Anderson
If you are unfamiliar with what the Pg/E2 (progesterone to estrogen) ratio is, it is something many physicians use when a woman suffers from hormonal symptoms, yet their lab results appear to be within the “normal” range.
I won’t go into the exact calculations as of now, but essentially in both saliva and blood tests, you are aiming for a progesterone to estrogen ratio of 100-500. (To calculate your progesterone to estrogen ratio, take your progesterone and divide it by your estrogen which then provides your progesterone to estrogen ratio. Providers vary but I have observed many practitioners aiming at a progesterone to estrogen ratio greater than 200.)
When progesterone is low in relation to estrogen, then your ratio goes lower. This is what is termed estrogen dominance and is most common especially in women over the age of 40. This also suggests relative progesterone deficiency. (For more on estrogen dominance, read my article here.)
When progesterone is high in relation to estrogen then it is described as progesterone dominance. This also suggests a deficiency of estrogen relative to progesterone.
Symptoms of Progesterone Deficiency (aka Estrogen Dominance)
Mood changes
Anxiety
Nervousness
Irritability.
Depression
Migraines
Hot flashes
Low libido
Menstrual problems (short, long, heavy, irregular)
PMS
Menopause symptoms
Standard Natural Treatment For Optimal Progesterone to Estrogen Ratios
This is where I am going to part ways with many natural doctors or better stated semi-natural doctors. In 2018 the standard “go-to” treatment for estrogen dominance is hormone replacement therapy (HRT) using progesterone to increase progesterone while leaving estrogen the same and thus improving the Pg/E2 ratio. While not everyone is doing this, the vast majority are.
The standard treatment for Progesterone dominance is to use HRT to provide additional estrogen and thus fixing the ideal ratio (100-500).
(I also note that this is an oversimplified example but illustrates the point.)
The PROBLEM!
I personally have a problem with hormone replacement therapy and I think you should too. The problem is that nobody seems to be asking the deeper question of why these ratios are off in the first place! Why in 2018 do so many women need HRT when in even as recent as the year 2000 you were hard pressed to find a women on HRT?
I thought natural practitioners were supposed to be looking for the root cause?
What happened to the days when the physician would dig deep into their wisdom and knowledge base for answers rather than simply prescribing “natural” hormone replacement therapy? If you are missing your ovaries and or uterus, or have other extenuating circumstances then there may be a valid reason for hormone replacement, but otherwise the most natural way to balance your hormones permanently is to avoid adding hormones altogether.
In a subsequent article I will address all the negative side effects of HRT, but for now, know that the biggest problem in my opinion isn’t cancer risk, but rather that it forgets to dig into the WHY and look for a root cause, thus it makes it much like other prescription drugs that only address symptoms. (Yes, I realize that this is a highly controversial statement.)
How to Correct Your Ratio 95% of the time
I get the opportunity to work with a lot women in my practice. Most women don’t come in complaining of hormonal imbalance, yet most have an imbalance that appears during the course of treatment and what I find 95% of the time is that what shows up in the treatment process is high estrogen. The other 5% is low progesterone usually due to excessive stress.
So… if I was a female at home reading this article and guessing which was causing my symptoms regarding libido, hair growth, cramping, tenderness, mood swings, etc. I would guess it was high estrogen.
In fact I would go so far as to say that, even if you are a female that has blood or saliva labs from your doctor that suggest your estrogen is low or even “undetectable” I would still suggest that you are much more likely to have estrogen excess and/or estrogen dysregulation than a true progesterone deficiency.
This does not mean that you shouldn’t treat your progesterone to estrogen ratio, it just means that in my opinion, the best way to balance your Pg/E2 ratio is to lower estrogen almost every time. …More




 I lost about 3 or 4 Lbs at the beginning then my weight didn’t change, but i do think I might have lost fat mass as trousers seemed to get easier to put on…
I lost about 3 or 4 Lbs at the beginning then my weight didn’t change, but i do think I might have lost fat mass as trousers seemed to get easier to put on…

