This statement seems odd to me. When I consume excess protein I get hot and there is also the higher thermic effect of protein. I am not sure if those are actually the same or if getting hot is essentially raised metabolism and the thermic effect of food means that a higher number of calories are being burned while dealing with the protein.
The statement seems to make sense if it was carbs instead.
I am not saying the statement is wrong - just that 100 excess calories of protein will result in less storage (i.e. not produce 100 calories of fat on the body).
That may be in-line with my theory or hypothesis (et al.); your burning it directly (UCP-1) as energy via BAT or brown adipose tissue or the browning (iron) of WAT or white adipose tissue and at the same time burning the VAT or visceral adipose tissue off the internal organs and not storing it as glycogen or fat?
A 24 ounce Ribeye (i.e. over consumption) will have over 600 calories of protein. I think extra heat and the thermic effect will cut into that but, I don’t think you’ll completely avoid some storage. (Of course, not a doctor, so don’t know if protein not dealt with immediately in one of these ways wouldn’t just be excreted anyway - directly supporting your hypothesis.)
I love Dr. Fung but this statement by him is lazy and similar statements by others have led to the whole “excess protein is fine because gluconeogenesis is demand driven.” line of thought.
What is should say is:
“Any protein eaten in excess needs to be converted to glucose, fat for storage, or deanimated for their carbon skeletons and consumed as fuel.”
The “gluconeogenesis is demand driven” people are right. Only a small percentage of consumed protein is used for gluconeogenesis. However a large percentage of excess protein is burned for energy since it cannot be stored. Every molecule of ATP generated from consumed protein is one that isn’t generated from the products of lipolysis.
Excess protein behave similarly to alcohol. It has a tiny storage pool (alcohol has none) and so it has priority in being burned as fuel over carbohydrates and fat.
I think @Iced is correct. They do recommend exercise be performed while fasting. They say it suppresses muscle loss.
There is also a lot of evidence now that exercise itself promotes autophagy. For this reason alone it makes sense to pair with fasting if your aim is to prevent loose skin.
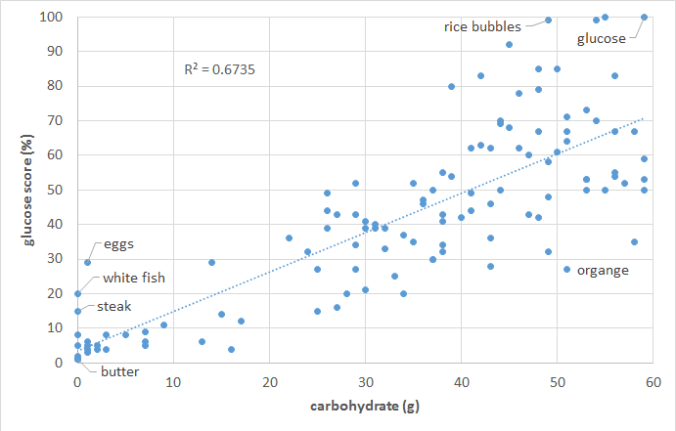
The food insulin index testing measured the glucose and insulin response to various foods in HEALTHY PEOPLE (i.e. non-diabetic young university students).
To calculate the glucose score or the insulin index pure glucose gets a score of 100% while everything else gets a score between zero and 100% based on the comparative glucose or insulin area under the curve response. So we are comparing the glucose and insulin response to various foods to eating pure glucose.
As shown in the chart below, the blood glucose response of HEALTHY PEOPLE is proportional to their carbohydrate intake. Meat and fish and high-fat foods (butter, cream, oil) tend to have a negligible impact on glucose.…More
As I wrote before, if you are trying to fast and strength training drives hunger, it would be worse (in my opinion) to eat (killing long running autophagy) or to have to suffer too much (likely hurting long-term compliance when a lot of weight loss is needed).
Specifically on the “exercise itself promotes autophagy”. My concern there is that if you are already strict water (plus electrolytes-only) fasting - autophagy is already in high gear. I am not sure that adding exercise will accelerate it more than incrementally higher (maybe maxed out so not at all(?) - I do not know). If the risks of the first point were a non-issue then sure - more muscle is (much!) better anyway - but, if hunger due to exercise is an issue, it might be best to let the fasting adaptations alone do their thing and worry about exercise when within 10 or 20% of goal. (Just intuition talking here - we’re not in the “show me the science” section.)
Training does give me a hunger bump. But you don’t have to train every day. Fifteen minutes of high intensity resistance training once a week will be all the exercise one needs to keep one’s muscles growing. That is unlikely to burn more than a 100 calories and while one may feel a short term increase in hunger it shouldn’t last long. Well, it doesn’t for me anyhow. I’m able to work out when on a 24-36 hr fast without any problem.
If it is a problem though, it’s not hard to do one’s training on a non fasting day and to thus get the benefits of both types of autophagy.
I think there are probably very few people who’d deny the importance of some amount of protein consumption for the purpose of maintaining healthy organs, bones, and muscles. I’ve yet to meet a “zero-protein” advocate.
So, yes, of course protein is vital, that’s not the question though. The question is how much is required to meet those needs as there is no benefit from exceeding them but plenty of downside risk to burning protein for energy, decreasing insulin sensitivity, and elevating growth factors such as mtor, insulin, and IGF-1.
What each of us should be aiming for is consuming a level of protein that is as close to exactly meeting our personal needs for it as possible. Thus, if we are talking to a 5’3 woman who doesn’t exercise we shouldn’t be telling her that 100 grams of protein is just fine even though her macro is 40 grams.
I agree that we shouldn’t “fear” protein. But like many other thing in life, you can have too much of a good thing.
I agree.
A while ago in my endless search for a way to reverse my diabetes I tried a high protein low fat low carb diet. I developed high insulin levels and became very illl…but my blood glucose levels were perfect!
Took me about 8 months to figure out what was happenning. I looked great, dropped a lot of weight by just soldiering on…but ended up bed ridden cause I was just totally fried and felt like I had flu all the time.
Was working out twice a week with a brilliant exercise physiologist. Put on a lot of muscle. High CRP too.
Now I eat as little protein as I think I can get away with and lots of fat.
This is very interesting. Can you tell me what the macros were like on a high protein diet that you are on? Also has your high insulin gotten better since you’ve been on a high fat ketogenic diet? How much protein do you eat these days?
I was on a high protein low fat diet about two and half years ago, I am not on it now. Someone commented to me recently how sick I was and I really was very ill in the end…I had no idea protein could stimulate insulin in the absence of high blood glucose.
I didn’t follow any macros on high protein low fat diet…I just ate a desertspoon of oatbran a day and biggish steak or fish for dinner and few boiled eggs for breakfast. Cup of green leaves for lunch, with extra fish or steak if I was hungry. I think I was having a teaspoon of fat a day.
2 Insulin has dropped through the floor since high fat keto diet and diabetes has totally reversed, no longer in the diabetic range at all.
3 Now I eat as much protein as I want to… but I also eat a lot of fat. I was stressing over measuring protein grams but gave up because the hassle factor was too high.
I fast frequently when I feel like it.
I eat 2 meals a day, lunch and dinner and usually have about a palm of steak (my palm) or a whole hand of fish (my whole hand) each meal. I add a tablespoon of butter to every meal I eat and usually some coconut oil as well or a few other oils.
Am about to test my omega 3:6 ratio to see how that is going.
I don’t track macros, I go by my appetite and measurements of my waist. I eat when I want and what I want as long as it is fat or protein. I avoid all sugars including stevia etc.
Thank you @anon13588705 for the details concerning your high protein diet. You really were very low carb (which is what I was wondering about, low carb can mean such a range of things) and so the culprit for your higher insulin must be the protein. I knew protein stimulated insulin production but this really demonstrates how dangerous high protein can be for those who already have hyperinsulinemia.
It sounds like we eat similarly. I generally eat once a day. I’m currently carnivore though and I think my protein consumption has gone way up. I’m not happy about that as it seems to leave me hungrier, much as carbs do, and also I just really do believe it’s not good for long term health. I’m working on bringing my fats closer to 80%.
Congratulations on reversing you diabetes. That’s a great accomplishment.
To be honest I find it so hard to actually count how much protein in getting. I like the Palm sized analogy… this kind of info is helpful for people starting out.
I heard Stephanie keto person recommending a palm sized portion of meat with three handfuls of veg and a couple of tablespoons added fat.
I heard Eric berg talking about it and saying that 3-6oz per meal is enough… I think he meant of meat so this would equate to around 100- 150g of meat which depending on how lean it is would be at most 30g protein.
Higher blood sugars on higher protein might not be so bad post prandial? Thinking this is ”dangerous”MIGHT not be such a good idea? A blood sugar/glucose spike is not the same as chronically elevated levels of insulin? I sure hope someday somebody will develop a machine that can measure insulin levels on the fly?
Looking at Hyperlipid’s blog post, you begin to wonder what is “normal” for a person who is doing a Ketogenic diet long-term and the testing standards that are considered “normal” by laboratory standards for high octane sugar burners?
Confusing?
Hyperlypid: “…The general opinion in LC circles is that you need 150g of carbohydrate per day for three days before an oral glucose tolerance test.
I did this carb loading thing, then performed my own OGTT. It came out very normal except for mild reactive hypoglycaemia.
So, I often walk around with a fasting blood glucose of 5.9mmol/l and in mild ketosis, yet have normal pancreatic and muscle function, provided I carb load before the test. BTW my FBG dropped to 4.3mmol/l after three days of carb loading.
That then raises the question as to whether Mark “iwilsmar” and myself are typical of LC eating people, or an oddity or two.
This brought to mind the self selected macronutrient study performed on mice by Ortman, Prinzler and Klause. They allowed mice to select their own diet and, lo and behold, the mice chose (by calories, not weight!) 82% fat and 5.6% carbohydrate. Sensible mice.
NB These German mice should each be given Professorships of Nutrition at medical schools in the most obese nations of the world. Quite what we should do with the current professors I’m not sure, but I bet the mice could think of something.
Anyway, these mice are cool. The only thing that bugged me when I first read the paper was that they had a higher fasting blood glucose than those poor mice fed the normal junk which passes for laboratory mouse “chow”.
This now fits in to an overall pattern. Elevated non esterified fatty acids induce physiological insulin resistance and a higher than expected FBG level. A simple switch to higher carbohydrate eating (in myself) allows the normal underlying pancreatic and muscle function to show. It also fits in with the FBG of 3.5mmol/l found in the carbohydrate fuelled natives in the Kitava studies.
[1] Chris Kresser: “…To put the most accurate picture together, I like to have all four: fasting blood glucose, A1c, post-meal glucose and fructosamine. But if I only had to choose one, it would definitely be post-meal glucose. …” …More
[2] Diabetes: Are high blood glucose levels an effect rather than the cause of the disease? Date: March 15, 2018 Source: German Cancer Research Center (Deutsches Krebsforschungszentrum, DKFZ) Summary:
Insulin resistance and elevated blood glucose levels are considered to be the cause of type 2 diabetes. However, scientists have now provided evidence that things might be completely different. They showed in flies that elevated levels of the metabolite MG (methylglyoxal) cause the typical diabetic disturbances of the metabolism and lead to insulin resistance, obesity and elevated blood sugar levels. …More
[3] Chris Masterjohn: “…Many people will be familiar with the fact that variation in red blood cell turnover confounds this measurement. Less well known is that variations in the deglycating enzyme fructosamine 3-kinase (FN3K) also confound the measurement. Counter-intuitively, if you have a higher rate of this deglycating enzyme but a lower rate of downstream metabolism of 3-deoxyglucosone, your lower Hba1c could actually mean MORE glycation . I conclude that Hba1c is a useful test, but only in the context of a bigger picture put together with more information . …” …MoreSee also his doctoral thesis:Regulation of Methylglyoxal Accumulation by Glutathione and Dietary Antioxidants (thesis paywalled)