@amwassil Thanks for the O’Hearn quotes.
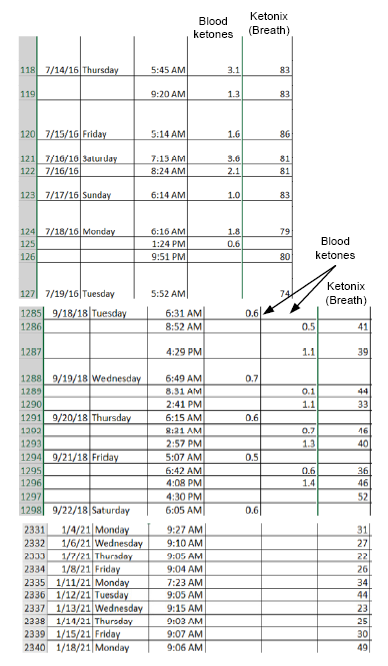
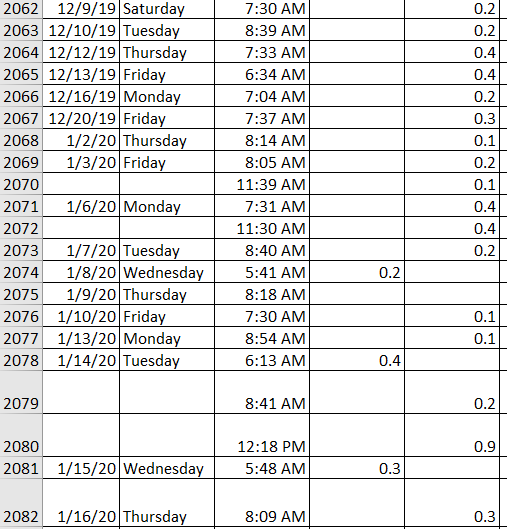
What she doesn’t explain is why this changes over time, although the diet doesn’t change much. If anything, I’m eating higher fat now than I did say a year ago, but my ketone levels are no higher (at least by Ketonix – have Precision Xtra strips added to my cart, but haven’t purchased them).
Now, I don’t have exact numbers (which wouldn’t be “exact” anyway), as I’m not weighing everything, but I am adding more fat to my lean meats to see what happens. Even ate lean beef (cold) with butter the other day.
To @FrankoBear’s point, though, I’m adding mainly MUFAs and still trying to add sat fat while limiting PUFAs. So, suet (mainly MUFA, but “high” in sat fat too), with A2 cheeses at times to up the sat fat, and some sat fat in the evenings (10% fat yogurt, sometimes with cacao butter).
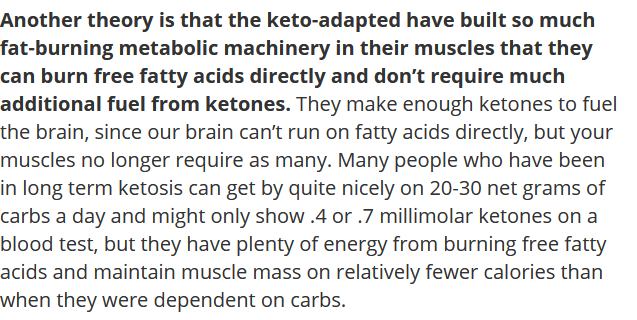
I’m still leaning to the FFA theory and my muscles directly using FFAs instead of ketones. This means that even if I did increase PUFAs, I wouldn’t get the same result in increased ketones now as I did say 3+ years ago. My body has figured out I don’t need the ketones as much.
Unfortunately, all I have right now to test is my ketonix (breath ketone analyzer), which is tough to interpret. Sometimes, it does seem like eating more fat the day before causes a higher reading; other times, not so much. And if calories factor in there, that makes it even harder to interpret, since I’m not counting calories.
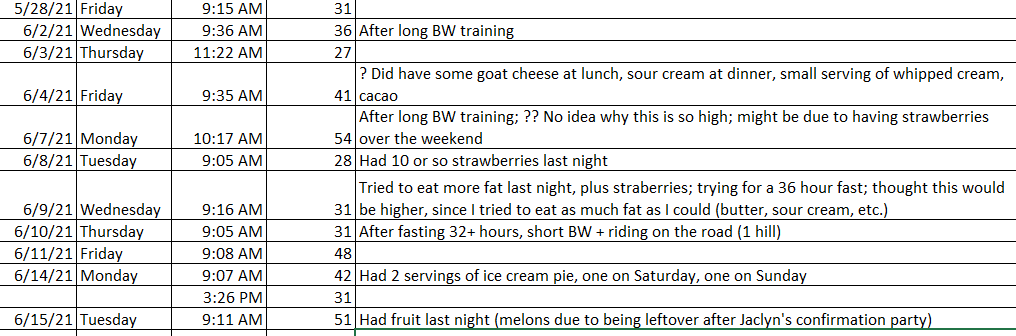
My ketonix readings vary from 21-51 lately, still a far cry from the 70-80+ a few years ago. And as with many of my n=1 tests, the results I thought I would get often don’t show up. See June 9, when I tried to eat high fat the day before (due to wanting to fast, and subsequently doing so). Thought I’d get higher results, but didn’t. Lots of data points here I thought would be different.