
Again, don’t get too excited about Lp(a) (or ApoB for that matter). My last two Lp(a) tests:
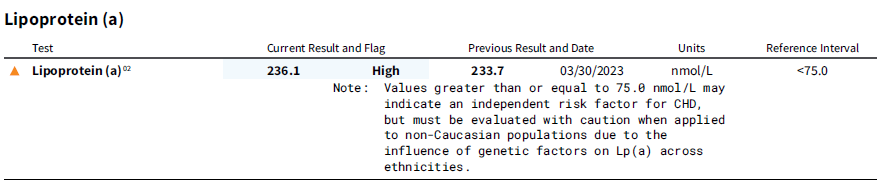
Those levels are somewhere around the top something % of people (the “something” changes depending on study). And I have around that value for the last 10 years, since I got the value tested.
After 5.5 years, my CAC scan score was zero. At least from a “hardened” atherosclerosis as measured by CAC scan, Lp(a) doesn’t seem to be causing this.
Moreover, there’s not much you can do about high Lp(a). Statins increase Lp(a), at least in some studies. You can take a PSCK9i, but even these only lower it so much, maybe 27% or so:
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.118.037184
But take a look at this figure from the supplementary material:
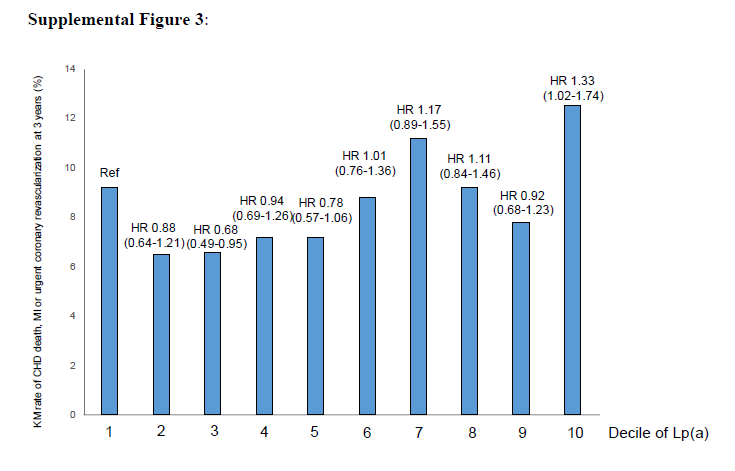
If Lp(a) was the deadly killer it’s supposed to be, this shouldn’t be a flat line, which is basically what it is. Ref is the lowest decile, and only two lines are above that.
As for ApoB, I know one can find studies where ApoB is a terrible marker. I was following someone on Twitter who had a ton of studies showin ApoB was not a great marker. Unfortunately, I don’t remember who this was and can’t find his information.
 I have/had super high, and I mean high cholesterol since before I ever got on Keto. I remember one time it was 300, and I went on this Oatmeal and niacin thing, it went down very little. Got on Keto, January will be 4 years, and my last Lipid Panel, total cholesterol was 500 something.
I have/had super high, and I mean high cholesterol since before I ever got on Keto. I remember one time it was 300, and I went on this Oatmeal and niacin thing, it went down very little. Got on Keto, January will be 4 years, and my last Lipid Panel, total cholesterol was 500 something. They’re stupid in my opinion because they just ignore the tests that come back “clean” but still want to pump me full of Big Pharma’s drugs. No way.
They’re stupid in my opinion because they just ignore the tests that come back “clean” but still want to pump me full of Big Pharma’s drugs. No way.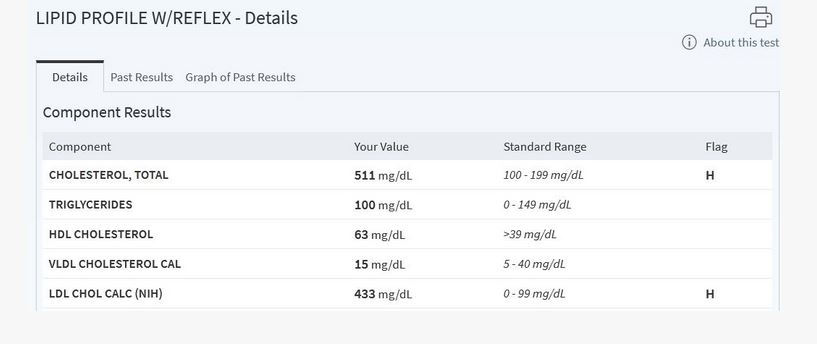





 Of course all she can do is talk to her doctor, I told her she needs to ask the questions she’s asking me, to her doctor instead
Of course all she can do is talk to her doctor, I told her she needs to ask the questions she’s asking me, to her doctor instead 
