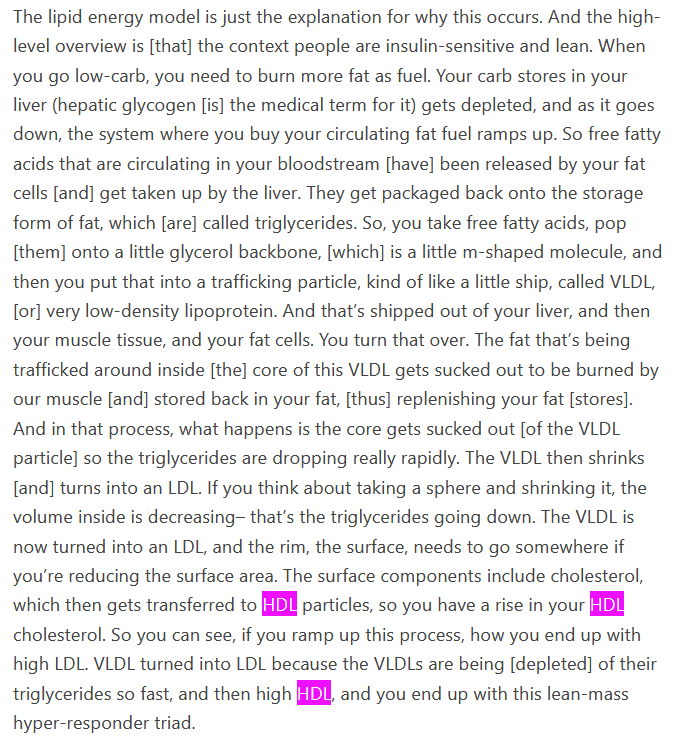
That passage you quote is closer to what I understood to be going on. However, that bit about cholesterol being transferred from LDL to HDL is news to me, though it certainly makes sense. And I notice that it’s the cholesterol from the lipoprotein container that he seems to be talking about, and I only recently learned that there was cholesterol in the container, which, again, is not surprising.
I’m not versed in what is supposed to go on generally for everyone versus what happens specifically to LMHR’s. It gets confusing, because some lipid numbers are usually calculated, rather than measured, and I’m not clear whether chylomicrons are separate from VLDL, or whether they turn into VLDL. I believe I may have heard both. One understanding is that chylomicrons carry the energy (as fat) from the current meal, so if they turn into VLDL, then that would explain high triglycerides. But Feldman makes it sound as though VLDL is carrying fatty acids from adipocytes in the case of LMHR’s, but does that mean that the liver makes the VLDL but then they go and pick up more triglycerides from the fat cells?
In any case, the contents of chylomicrons do not appear in lipid results if the blood draw was done fasting, because they have a very short dwell time. But what if the patient forgets and eats before the blood draw? If the chylomicrons and the other LDL are all the same lipoprotein, there might not be any way to distinguish between them. (HDL is supposed to have a different type of lipoprotein as its container.) That might inflate the triglyceride number, mightn’t it?
To quote Moonstruck, “I’m so confused!”
ETA: It does seem to make sense, as the Norwood paper you linked posits, that lean people would have higher LDL and HDL, since there would certainly be a greater need for shuttling triglycerides around the body. They would be taken to cells needing energy by the LDL and returned to the liver in the HDL (according to Feldman, the cholesterol is merely along for the ride). So eating in a way that minimises fasting triglycerides would certainly promote this. And most of the rest of us are probably fat enough that our LDL doesn’t need to work nearly as hard.


 It really burns me up because I know they’ve done none of the tests for FH on me at all!
It really burns me up because I know they’ve done none of the tests for FH on me at all!