Trying to rock this low-carb/keto lifestyle but my labs just came back:
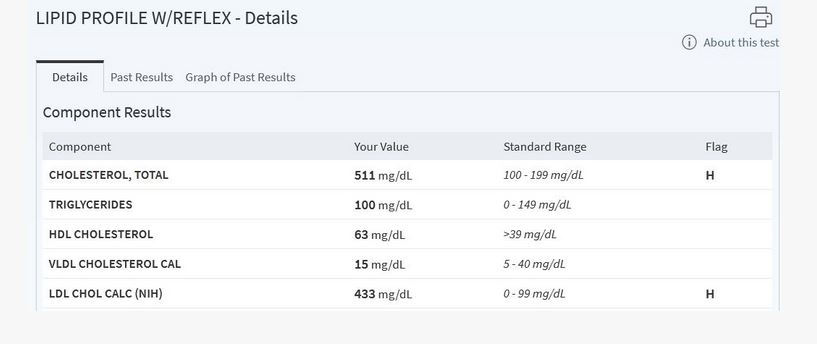
LDL cholesterol went up from 170 to 220
HDL went up from 46 to 70
Trigs went down from 70 to 49
No health issues otherwise and not taking any meds. Now doc wants additional testing like Calcium score and LDL particle test. Hopefully it’s going to look good since I’m 36 and should be in the clear. I’m doing this for about 4 months and have encountered several benefits since drastically reduced carbs.
My question is, who of you here has similar labs and has lived without any issues for longer than 5 years? No issues meaning no heart related disease for 5+ years on this WOE? I’m female so hopefully I’m not the only one here with this type of dilemma.
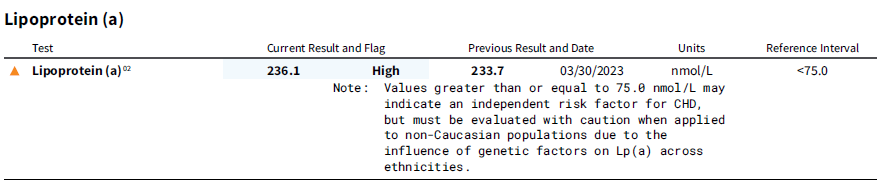
I’m familiar with LMHR and believe I might be one of them, but as you know all that is very new and there’s not much data to support that high LDL is harmless in low carb eating individuals (which by the way I do believe to be true since there is lack of inflammatory foods etc).
I do not want to take statins and never will. But I’m also wondering if this is truly fine 
Thank you all for reading.


 They’re stupid in my opinion because they just ignore the tests that come back “clean” but still want to pump me full of Big Pharma’s drugs. No way.
They’re stupid in my opinion because they just ignore the tests that come back “clean” but still want to pump me full of Big Pharma’s drugs. No way.