
@OldDoug @Karim_Wassef Thank you Gentlemen. Your posts were both clarifying.
Karim's Extended Fast Tracker - come along for the ride
Karim_Wassef
(Karim Wassef)
#863
I agree. GKI is meaningful in context.
It’s only a shadow of a shadow of what we really want to measure … insulin and glucagon… mTOR and AMPK… or actual autophagy.
Fasting is the easiest to contextualize … No exogenous sources. So for my experiment, it’s reasonable to assume autophagy.
With macros inbound, it gets complicated… I do wonder what a very high fat, very low protein, no carb diet would do.
Even then, some protein while in deep keto releases glucagon instead of insulin… so what happens to mTOR and AMPK? And what is the periodicity required to repeat this response?
Karim_Wassef
(Karim Wassef)
#864
I use this one
GreaterGoods Bluetooth Connected Body Fat Bathroom Smart Scale
I compared the results to my DEXA and it lined up much better than I expected with the confounding factor being hydration. Water is very heavy compared to fat and the biology of hydration into fat, organ and muscle tissue means that a lot of “weight” is meaningless unless the effect of water is taken into account.
So I take the measurement first thing in the morning after elimination of water and waste. At least that helps me keep the data relatively comparable if not absolutely accurate.
RightNOW
(PJ)
#865
Thanks. Since chronic edema (heart valve adding it, diuretics removing it) is the bane of my body, I guess a scale like that wouldn’t work for me, though at my size it probably doesn’t matter right now anyway.
I’m glad to hear those are getting better though!
OldDoug
(Doug)
#866
I’d like to see a study where they measured human autophagy while totally fasting versus eating only fat, to see what difference it makes. My gut feeling is that eating fat wouldn’t make much difference, i.e. while fasting we’re consuming our own fat from storage anyway. I imagine there is some stimulating of hormones in the stomach and small intestine from eating fat…?
Eating protein drastically affects mTOR and AMPK - even the very small amounts of protein the body gets from autophagic processes act on them, so to an extent autophagy is self-regulating.
Karim_Wassef
(Karim Wassef)
#867
I like data. Even if it’s not 100% accurate, it can generate interesting questions, if not answers.
Karim_Wassef
(Karim Wassef)
#868
My ultimate goal is gaining muscle mass while losing fat through behavior and nutrition.
I have not found it because my hormones are not willing to point me in that direction. Others may be more fortunate.
My only solution is to slowly cycle between catabolic and anabolic states…
Don_Q
(Windmill Tilter)
#869
It depends on how you look at it I guess. Autophagy starts at a GKI of around 60. To put the magnitude of the autophagy achieved with a BG of 100 and a K of .1 into perspective, consider that normal protein turnover for humans is around 300-400g per day (citation below). The average protein consumption is around 60-80g per day. That 220g-360g per day difference between daily protein turnover and exogenous protein intake represents autophagy achieved while eating snickers bars and cheeseburgers as a “normal” SAD eating human!
I share your questions about GKI, but I would phrase them thusly:
- What GKI numbers mark the transition from normal autophagy to magical mystery authophagy?
- What are the specific categories of magical mystery authophagy?
- Which kinds of magical mystery autophagy shorten life span?
- Which categories of magical mystery autophagy are harmful?
- Which kinds of magical mystery autophagy are beneficial?
- Does GKI correspond to any of these categories or outcomes???
That last one is important. We don’t know the outcomes, and we don’t know how GKI corresponds to them. It’s voodoo at best. There is a general presumption that autophagy is uniformly good, and that lower GKI is better. The people who actually study this stuff (e.g. Vlongo) seem more than a little afraid of intensive autophagy, and recommend brief bouts quarterly at most (IIRC). I say this as someone who genuinely loves extended fasting. I’m not aware of any compelling evidence that frequent intensive autophagy is benign. I do it anyway.
Nobody really seems to understand autophagy or GKI, as far as I can tell.
https://www.sciencedirect.com/topics/biochemistry-genetics-and-molecular-biology/protein-turnover
Ilana_Rose
(mole person)
#870
@Don_Q yes, I agree. At first I was all “Oh wow, I guess I don’t even need to think about fasting since my GKI is already in the Dr. Boz “cures cancer” range.” But it makes no sense because of what @OldDoug has said. I’m eating protein. Protein doubly stimulates Mtor. Once directly from the protein and again from the insulin.
But I am starting to really wonder at whether I need fasting for sufficient autophagy anyhow. We simply have no idea what’s an ideal amount of autophagy. Obviously you can have too much. But how much is that? Am I in a metabolic state with my super low glucose and insulin where I’m already ideal? Maybe fasting would be a negative. Who’s to say. At this point we just don’t have enough evidence. Right?
Don_Q
(Windmill Tilter)
#871
What do you think about the following strategy: lift heavy, followed by 2 days of feasting, followed by 1 day of protein sparing modified fasting (PSMF)? After all my hours of research, this is the best strategy can come up with when I get my BMI under 25.
You can capture around 66% of potential muscle protein synthesis in the 48 hours after lifting while in a hypercaloric, anabolic feasting state. You minimize catabolism with 125g of protein only (500 kcal) on your PSMF day. This yields around 6lbs of fat loss a month, and net muscle gain, while keeping you metabollically happy from an RMR, gherelin and leptin standpoint.
My understanding is that deep autophagy eats 150g (5oz) of lean mass protein per day for a man with a sub 25 BMI. A shit-ton (non metric unit) of that is skeletal muscle. It sure as hell isn’t all loose skin. Assuming that were all muscle (it’s not obviously), it might over a week of lifting and feasting to replace each days worth of deep fasting muscle loss. Deep autophagy and muscle gain seem like poor bedfellows.
I’d be genuinely thrilled to be wrong about that though. Last year’s 19 day fast seems like an interesting case study. How long did it take to regain lean mass losses after the 19 day fast based on your Dexa baseline and follow ups?
If it seems like I’m being dismissive of your current undertaking, I’m not! I have a great deal of respect for the tenacity it requires, and I don’t have a clue what other benefits fasts of this duration might confer. All I’m saying is that on the surface it seems at odds with the quoted objective (net muscle gain annually) based on my (very) limited understanding of this stuff.
OldDoug
(Doug)
#872
Ilana, I don’t know all of what Dr. Boz was saying, but I’d think that some lesser cancer risk would be attributable to lower blood sugar and insulin alone. Some types of cancer grow faster in a higher-sugar environment; has nothing to do with autophagy. Yet there’s a lot we don’t know and some confounding things - I think at least one cancer type is increased by autophagy itself… Dr. Boz/GKI Index doesn’t apply in the same way to people on keto diets since there’s not the massive change/reversal in glucose and ketones as with heavy carb-eaters going into the fasted state.
Taking that sentence by itself, I’d certainly think that on that score you’re perfect or nearly so. No likely reason at all to change.
Yes, we’re still guessing about a good bit of it all. I wonder about “too much autophagy,” however. People that have done very long fasts - 100, 200 days, even over a year - don’t display anything that would make one think they had too much.
Different tissues have different rates of autophagy increase and methods of stimulation. Exercise itself increases autophagy in skeletal muscle; diet notwithstanding. Much of the nervous system is supposed to have a low rate of autophagy constantly occuring.
If one has no conditions that autophagy presumably would or could remedy, and no family history or personal expectation that trouble may lie ahead, then perhaps they don’t “need” to increase autophagy. I would hesitate to really assert that, though.
If we otherwise live long enough, about 1/3 of us get Alzheimer’s Disease. Add in other types of dementia and other often age-related neurological impairments, and I’d say there’s a strong argument for fasting at least a few days a few times per year, if not every month. Those are guesses on my part - it seems like we’re light years away from really being able to quantify the risks/rewards, probable improvement due to fasting, etc.
Don_Q
(Windmill Tilter)
#873
Good point. We are starting to get some more science linking fasting with specific (and important!) outcomes.
Vlongo is doing interesting work in this space. He just kicked off a long term study with 120 subjects diagnosed with Alzheimer’s, and placing one group on a monthly 5 day fast (his fat-fast protocol). Mattson is doing a similar study with a 5:2 feast/fast protocol. Those results will be fascinating to read. Hopefully they’re tracking glucose and ketones.
Karim_Wassef
(Karim Wassef)
#874
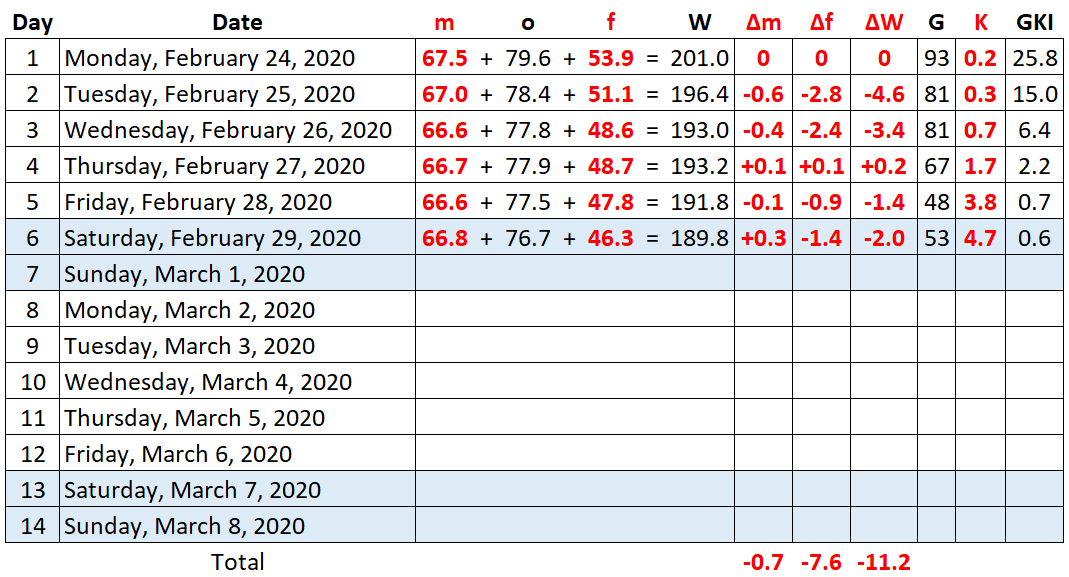
Day 6 final
So many comments to respond to 
This fasting may seem at odds with my goal but it’s not when you see it in the context of the full year. I’ve been eating heavy protein and fat while on keto + lifting heavy. So I’ve managed to build up some muscle and a nice layer of adipose fat… So I’ve had my anabolic phase (bulking) and now this is my catabolic phase (cutting).
I also do expect that fasting autophagy does have other curative properties as the body drives into a unique state focused on removing unnecessary, unhealthy and potentially life shortening elements (lab rats live nearly 2x while in this state). I don’t have any ailments that I’m aware of, but I also don’t know the length of my telomeres or the mass of my visceral fat (since my last DEXA). This state will reduce inflammation and that alone has benefits… It also increases testosterone and that’s important in regenerating muscle mass as I get older.
After the last fast, I moved into a moderate protein high fat vegan stage (for lent actually) and I recovered my muscle mass in about 2 weeks.
Karim_Wassef
(Karim Wassef)
#875
I can try it again after the fast. I’ve tried cycling protein and fat but it hasn’t been effective in the past.
Ilana_Rose
(mole person)
#876
I was actually being a little facetious in my reference to the Boz ratio. She claims that you get certain specific results at certain ratios and she really lacks any good scientific evidence for her claims. Here is a chart:
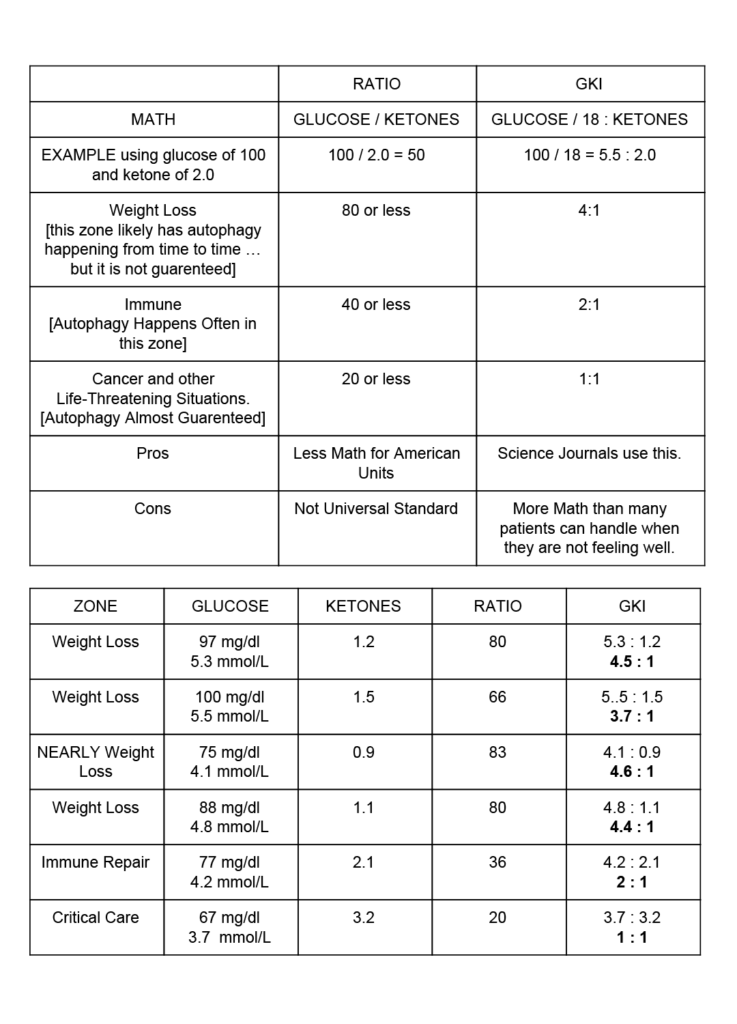
According to her, high level autophagy is “almost guaranteed” at a GKI of one and is useful for controlling cancer spread and immunological issues.
Yes, but that’s not the claim. Rather it’s for actual control of cancer spread.
This isn’t her claim though. She, and other people suggesting that GKI is useful in cancer treatment, believe that the metabolic state of the GKI itself represents is what’s operative not the change from a high to a low GKI. I’m not saying that it wouldn’t be helpful for cancer treatment, I actually think that there is preliminary reasons to think that it might, but I don’t think that we have any good reason to think that benefit is a result of autophagy. It seems much more likely to be a direct result of a low glucose metabolic environment.
These people are pretty much all people with significant weight to lose. Dr. Fung makes a point that I think is relevant to this. People who are actively losing fat need much less exogenous protein because they are daily losing some protein need to support all the extra fat. But what happens during fasting for lean people like myself? Every day without protein must result in lean loss just to feed my bodies glucose needs. In other words how much extra autophagy a body can handle might be dependent on how much protein there is to lose endogenously.
I guess this is one of the reasons that I wonder about where the “healing” effect of the lowered GKI is actually coming from. I’ve had enormous healing from a deeply ketogenic diet. My virtually permanent migraines are gone, and two seperate autoimmune attacks on my nervous system have gone into remission. But I never fast as it’s just been far too hard at my weight. I get so hungry that sleep is actually impossible.
Further, Paleo-Medicina treats all sorts of serious autoimmune, cancer, and gut related problems with an ultra low GKI diet but actively discourage their patients from fasting and have patient outcomes that are similar to my own. So really, how do we know where the “healing” is coming from?
But do a third of us on a deeply ketogenic diet who are constantly in a low glucose state get Alzheimer’s? It seems unlikely if the disease is actually a disfunction of glucose metabolism as is thought. And this raises the question again that perhaps the need for extra autophagy is greatly reduced in a very low glucose metabolism.
Anyhow, just my musings.
Karim_Wassef
(Karim Wassef)
#878
Day 7
As I fast, I get several recurring symptoms that I need to work through. This morning, the “gurgling” was intense.
This isn’t the effect of hunger or even a desire for food. It’s just a sound and feeling of liquids and gases moving throughout my digestive system. It eventually ends by being eliminated as liquid waste but that’s to be expected given that the intake is liquid only.
Today, the movement was intense though. It sounds like someone is filling a large container with water and then emptying it… and while filling it, it’s from a height to cause substantial agitation and bubbles to form… I realize it’s a poor description but that’s the closest approximation I have.
I suspect that this is a biproduct if the biofauna dying and being eliminated as well as some of the inner lining being flushed out with it. I still take ACV with my coffee but that culture is probably not viable without any fiber.
I don’t feel weak but I am experiencing the “slow” and “chills” of fasting. This happens at the same time as a continuous sustained feeling of energy build up. Slow and energetic seem at odds but that’s what I feel. I can do anything I need to but all actions are at a controlled pace. No explosive burst energy.
I think this is result of low glucose and I’m fine with it. Considering using my elliptical today to get some slow cardio in.
Ok. First results coming up in a bit.
Karim_Wassef
(Karim Wassef)
#880
Reduced inflammation, low glucose and low insulin alone are power contributors to health and healing. It’s why I started keto in the first place.
Weight loss/gain is a symptom not the cause of the affliction. Heal the body, then the weight will follow.
I don’t know how fasting healing compares to protein sparing keto or regular keto… I find the GKI meaningful since it tracks with the results I’m measuring… but it may have deeper impact that we can’t measure.
Ilana_Rose
(mole person)
#881
Ah yes. Inflammation. I always forget it but I’ve reduced it so much on this diet. I didn’t realize how much it was a problem until it was gone. I’ve found a physical cue that tells me when it’s increasing now and if I act quickly I can generally reduce it again before it aggrevates my conditions.