Hmmmmm, treatment with a 50 year old drug plus some vitamins, or a multi-billion $$$$ vaccine? Not a one-time vaccine either like polio, but one you may have to take at least yearly, if not more often.
John Campbell’s usually pretty sensible, but he really messed this one up. Hard to believe how many people don’t spot some obvious errors or check out the Belgian “study” itself. I imagine that peer-review will dismiss the Belgian analysis, if it comes to that (I think the reviewing committee or individuals would basically say, “Fix this and re-submit it, if you want serious consideration”). Looking through the YouTube comments, almost nobody bothers to really read the Belgian analysis or think about it.
Doc Campbell says, “I’m on pretty thin ice here…” but little does he know just how thin.
11+ minutes in, he’s talking about “no difference in baseline characteristics.” Well, he should have read all the way through - that’s not true, and it’s an enormous, serious flaw. Has no one else spotted it? This is the study-killer, as I see it.
Some other quibbles, less major - just before 14 minutes he begins talking about the hazard ratio. “If you had 100 patients surviving in the hydroxychloroquine group, you would have only have 68.4 surviving in the other group.” That’s really not what this means. The hazard ratio usually refers to death probability. If we are talking about survivors, then if things are 1 : 1 they are equal, i.e. or 100 per-capita survivors in one group would be equaled by the same in the other group.
Doc Campell has it as 100 versus 68.4, a 31.6% difference. But look at what it really is - it’s 100/88.6, an 11.4% difference. Before we even get to the study, he’s got it sounding like things are almost 3 times worse for the non-HCQ group, versus the HCQ group, than they really are.
Just after 19 minutes in, he says, “The theory for hydroxychloroquine and the theory for azithromycin are both good, the theory’s there.” Well, he ought to think a little more about the Belgian analysis, to begin with. Beyond that, the analysis also noted that the death rate for hydroxychloroquine and azithromycin was a little higher than for just hydroxychloroquine alone. So, hey Doc, hello…
Never had a blood test for Vitamin D that I know of, but same here - been taking Vitamin D (the D3 thing) for a good while now. No matter what else, it does look like you don’t want to go into fighting off the virus while being deficient.
I don’t know about this one. If the world had responded differently, better - like the way things were handled with the first SARS (some differences between the viruses acknowledged) - then things would have been better for a LOT of people, and I’d say that would involve more centralized control (or at least agreements). Not advocating for ‘one world gov’t,’ but fighting the virus has been pretty haphazard in a lot of places.
I read the whole thing, one time. Something doesn’t seem right with the “Independent predictors of in-hospital mortality.” It involves baseline characteristics, but I don’t think it’s a ‘fatal flaw’ in the study.
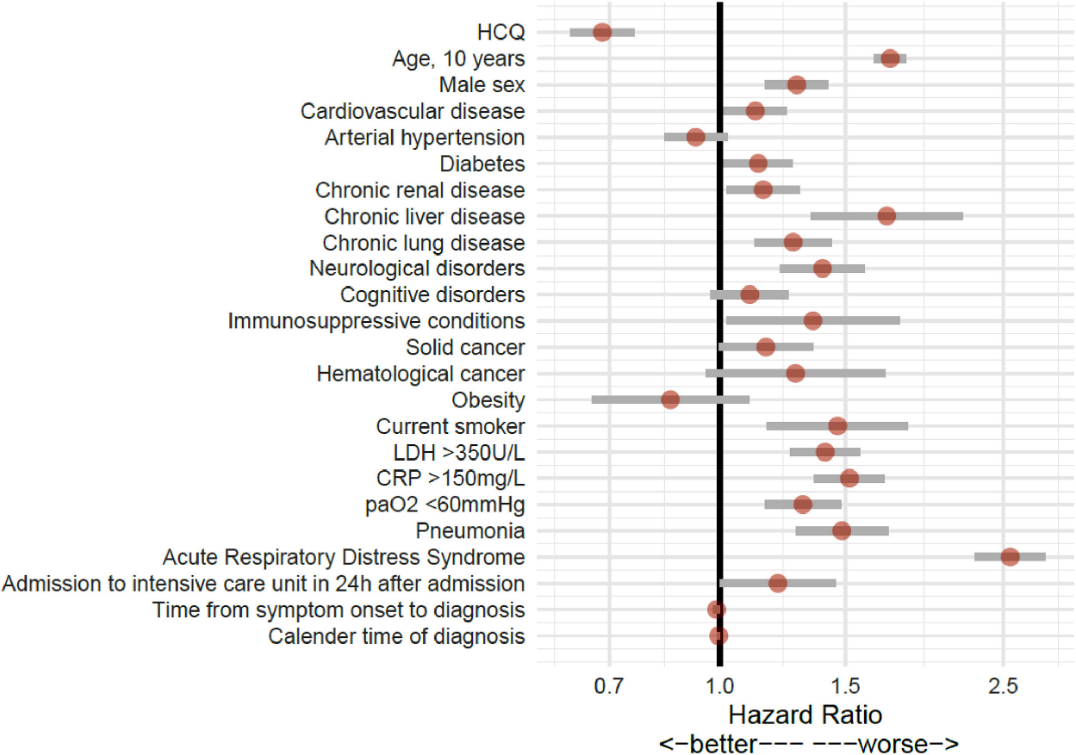
By now, it’s well-known that high blood pressure and obesity increase the risk, right? (If anything, I’d say the ‘obesity’ factor is the most under-reported and inadequately focused-upon thing.) The Belgian analysis has arterial hypertension and obesity decreasing the risk, so unless I’m missing something, there’s bizarre stuff going on.
It wasn’t a randomized controlled trial, just an observational analysis, so “some” degree of unexplained findings would be more expected. (The analysis notes that high blood pressure and obesity were significantly less frequent in the HCQ group, but while that’s one confounding thing, that’s not necessarily going to make for what looks like a real red flag to me.) But worst-case, it does call the conclusion into question. I didn’t see a breakdown of the dates of the administrations of the 5-day hydroxychloroquine regimen. The total period is over 2 months long. It would need to be pretty much the same as for the dates of the patients in the “non-HCQ” group. If not, then the potential for people with much higher inherent risk being in the non-HCQ group is there. Deaths accumulate - as one would expect - in patients with high blood pressure and/or obesity. Without “equal” time-of-administration for HCQ, then - even with selecting what seems like a fair mix of obese, etc., people for both groups, the HCQ group could include people with more innate resistance to the virus, and/or better overall received medical care, the later in the time period of the analysis they were. “Filtering out” (even if unintentionally) the ‘more susceptible’ people with certain conditions would leave the ‘less susceptible,’ and that is what the analysis’ “hazard ratio” chart shows.
In the “characteristics by treatment group” (Table 2) there is a note for ‘Obesity’ - it says, “Missingness is due to later onset of data collection.” Whatever that means… I don’t know - something does not seem to be right.
No actually it’s not. Again, very clear you don’t live here. If our checks and balances didn’t work than the US would have been converted to socialism and annexed to Europe while President Obama was running the show. He literally didn’t care what the house or congress would approve and said with a straight face he’d veto anything they wouldn’t approve and use executive power to do what he wanted. That’s a siting President with a LOT of power, and he still wasn’t able to bypass our system. It works just fine. Seems your issue is things being done that you personally disagree with.
If people are forming their opinions on the basis of that YouTube video or the Belgian study, then there’s a lot to be skeptical about.
I don’t see where they address this; weird. No alarm bells going off in their heads?
The Belgian study - Tables 1 & 2 are where it’s really at.
Table 1 - Characteristics by survival or non-survival are given for 8910 people - this includes those treated with a combination of things, including HCQ or other treatments specific to Covid-19. It gives a breakdown of survivors and non-survivors by age group and other characteristics.
Table 2 - Characteristics by treatment group (HCQ alone or ‘nothing’) are among 8075 people. It’s not the same overall group of people as in Table 1, and how this is not just ridiculous escapes me. It also just gives total deaths, not deaths by characteristic, as in Table 1, and that’s what we really need to see, the judge things.
Table 1 should also be for the 8075 people that the study is actually about. But it looks like the conclusion falls apart if they would have done it that way. Perhaps this is a case of “not being able to see the forest for the trees” thing? That’s being ‘kind’ and not assuming the writers are being deliberately deceptive.
Come on, guys - we all have opinions about politics, religion, etc. This forum is fairly loose about letting us all talk about all sorts of things, but there is a limit.
We knew it was 8075 people in the two groups, i.e. as I said - the larger group of 8910 includes those treated with a combination of things, including HCQ or other treatments specific to Covid-19. So why would they give us a breakdown of survival/non-survival for the larger group (which was not being considered)? All we care about is the HCQ alone people and the ‘nothing beyond standard care’ group (those who make up the 8075 people). It’s senseless to have Table 1 not be for those two groupings. Something is definitely not right.
Presumably they are giving a full report of what they did… firstly they looked at the 8910 then decided to restrict the numbers due to the reason given.
Looks to me like they are being completely transparent…
Maybe - I’m not sure. The way it’s presented does not make sense. We have two larger sets of people - the ‘HCQ and no-HCQ’ set of 8075 people, which the study is aimed at (and of course the study breaks that one down into the two smaller groups, respectively). Then we have another larger set of 8910 people, which includes multiple treatments.
The study is not about the 8910 people. It is about the 8075 people. Neither the study, nor the people reading it or reading about it - including us - really care about the 8910 group with the additional 835 people in it.
Table 2 gives good information about the 8075 people. What we need is the good information in Table 1 applied to the 8075 people, not the 8910 people. It makes no sense to address the 8910 people. It makes no sense to omit the Table 1 information for the 8075 people. The study is a comparative analysis, so let’s have the information for what is being compared, not for what’s not being compared.
Maybe it was just an oversight for the report writers and/or the researchers - that’s what I meant by a case of “not being able to see the forest for the trees” - perhaps they’re too involved with the details to see the proper approach as a whole.
They’re not giving us a full report of what they did - far from it, in fact. The study is about survivors and non-survivors, and HCQ or not. So let’s have that information - this is what’s in Table 1 - a breakdown by age groups and whether they lived or died, for the 8075 people. We need to see what the real numbers are and what adjustments the researchers made, if any.
This is important because there are large differences in the baseline characteristics of the HCQ and no-HCQ groups.
But the 8075 are a subset of the 8910 so they started out looking at the 8910 and then decided that there were confounders so just looked at the 8075 instead.
I think you are trying to find a conspiracy where this is simply transparency… I could be wrong but what would be the point in that.
If they already had all the data for the 8910 why not publish it?
They did that and then refined it to the 8075 that was more relevant to what they wanted to look at.
They began with 15,544 people and weeded them down to what they wanted. No reason to go into any detail about the characteristics of those excluded.
I’m not saying it’s an outright conspiracy, but it does appear to be shoddy thinking and nonsensical, in the end. Where they need to be transparent is with the information for the 8075 people that actually are in the study.
It wouldn’t hurt a thing. They can say anything they want about any group, but their error is in omitting information about the 8075 people that the study is looking at.
And if they’d given the information for the 8075 then all would be well, but they didn’t do that. They included stuff that was not germane, and left out needed things.
This is what I see as the fatal flaw in the Belgian study. I’d start by paying no attention to John Campbell’s botched analysis in the YouTube video. The researchers did make some adjustments - they ended up with an adjusted hazard ratio of 0.684. This is as opposed to the raw numbers calculation of the mortality of the HCQ group divided by the mortality of the no-HCQ group, which is 0.653.
<5% correction there, and look at the difference in the baseline characteristics:
The median age of the no-HCQ group was 11 years older. This makes an enormous difference. In the study, 90% of the deaths were among those aged 65 or older.
The portion of the no-HCQ group that was 65 or older was 36% higher than the portion of the HCQ group. There’s a study-killer right there.
Or, look at just the people that were 80 years old or older. 56.9% of all deaths occurred here. The portion of the no-HCQ group here is almost twice that of the HCQ group (44.6% versus 23.3%). Peer-review would address this immediately, i.e. “Get this rubbish out of here,” or “Fix it and come back with something rational…” etc.
As an illustration why such things are so egregious, let us consider that ≥ 80 years old group, and the total numbers of deaths in the study.
Deaths in the HCQ group were 804, with 957 in the no-HCQ group. If the rates of mortality between both groups were the same, there would have been 625 deaths in the no-HCQ group. (625 being less than 804 is due to there being less people in the no-HCQ group.)
So if we want ‘equality’ then the difference of 332 deaths (957 - 625) needs to be made up. From the study’s own tables, the ≥ 80 years old group had 56.9% of deaths. 1761 total deaths x 56.9% = 1002 deaths in the ≥ 80 years group.
Allocating the 1002 deaths between the HCQ group with the study as stated gives us 402 deaths for HCQ and 600 for no-HCQ.
Now let us make the percentage of HCQ patients be the same as was for no-HCQ: this means taking the study’s 23.3% of HCQ patients ≥ 80 years and multiplying it by 1.914 to equal the study’s 44.6% of no-HCQ patients. Taking the “as stated” 402 HCQ deaths x 1.914 = 769. The difference is 367 and we have already more than made up the 332 deaths for no-HCQ to have the same mortality as for HCQ (i.e. HCQ would have higher mortality, there).
Or, let us reverse the percentages, i.e. let’s put HCQ at 44.6% and no-HCQ at 23.3%. Now we have 2025 HCQ patients ≥ 80 years and 822 for no-HCQ. Using the study’s 56.9% death rate for ≥ 80 years old, that gives us 1152 dead for HCQ and 468 for no-HCQ. A difference of 684, again surpassing what we need for HCQ to have higher mortality, far surpassing it this time.
Either way, the study’s conclusion is easily shown to be false.
I can’t prove the writers had an agenda, but there are things that make me wonder. In the discussion/conclusion section at the end, they say, “In the context of the COVID-19 pandemic, HCQ therapy has been in the centre of debates, between hype and bashing, within and beyond the scientific community.”
“Hype” and “bashing” - this is unusual language for a purportedly scientific study. Definitely makes one wonder.
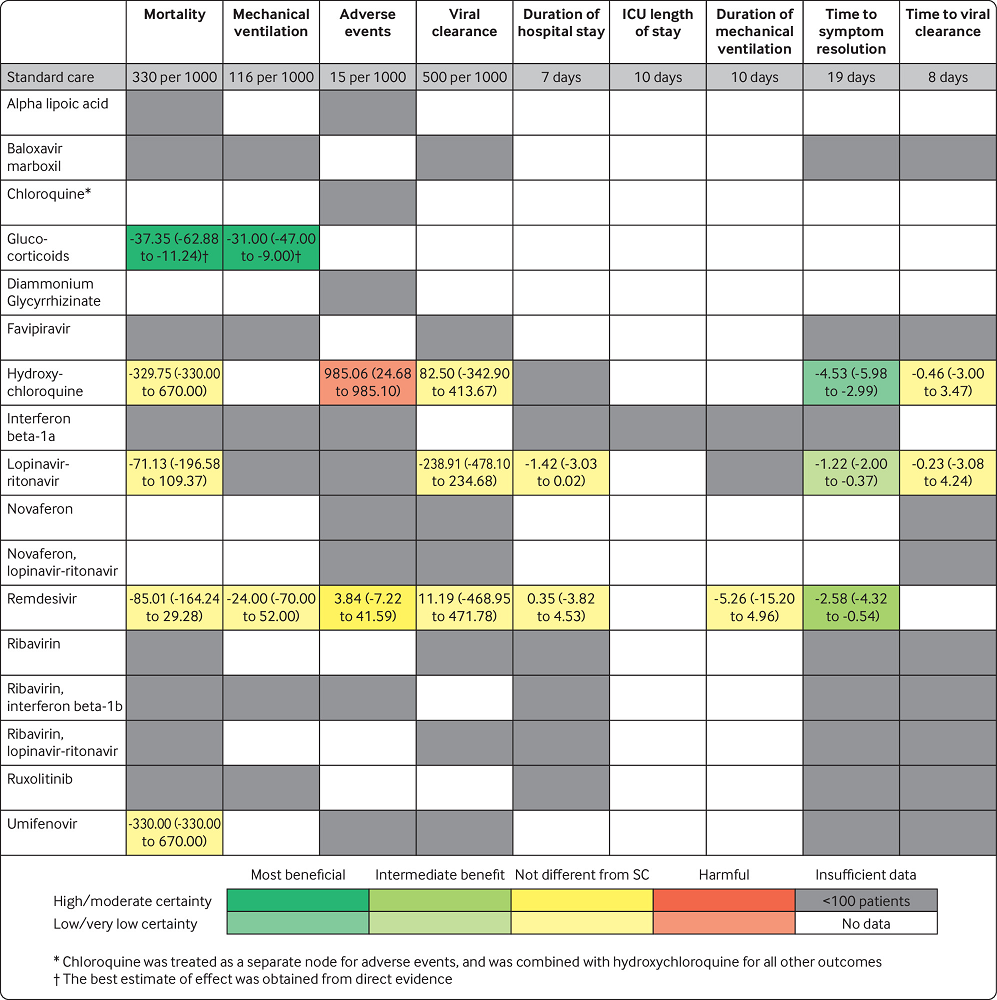
In their introduction, they say, “There is currently no robust antiviral or immunomodulatory treatment of SARS-CoV-2 infection, the causative agent of COVID-19.” This is dated in late August, 2020, and they’re somehow forgetting about Remdesivir, Umifenovir, Lopinavir, Ritonavir, etc. These are not “miracle cures,” but they’re certainly as “robust” as Hydroxychloroquine (even if we accept the Belgian study’s questionable findings).
The real question is not if Hydroxychloroquine can exhibit antiviral properties in a Petri dish (it can). Nor is it that it’s better than doing nothing, as far as drug administration for Covid-19, yet that’s the claimed focus of the study. The real question is if it can do the same or better job as other drugs, without bringing increased risk of harmful events due to the drug itself, and on the latter score alone is where Hydroxychloroquine gets ruled out.
The gross over-allocation of no-Hydroxychloroquine patients to the 80 years and older group in the study is quite damning. Just think if someone began with a “pro-Hydroxychloroquine” mindset, and then found out that the study operators chose things so that an age group with almost 60% of the total deaths (out of everybody) had almost twice as many people that received Hydroxychloroquine as those that did not.
They would be ‘screaming bloody murder,’ in effect, and rightly so.
I see another angle on this - the study admits that cardiovascular diseases were significantly more frequent in the no-Hydroxychloroquine group. This makes sense, as doctors were warned off using the drug in many cases - the study also mentions this fact, i.e. the ‘QT’ measurement for ventricular operations, etc.
Heart damage is a hallmark of Covid-19. Thus, the study was going to have a hard time being objective in this respect, alone. This was for good reason - the risks of Hydroxychloroquine are known and real (doctors don’t want to give it to some people), but the fact remains that there are many questionable aspects of the study.
The study also ‘talks itself up’ more than normal, deeming itself “robust,” etc. It’s as if they have a guilty conscience and/or are trying too hard. I would like to see a proper review by real academics with experience in such studies.
Occam’s razor - the simplest explanation is likely the best - the omitting of the Table 1 information for the study groups cannot be accidental or merely an oversight. The writers of the study report knew that if readers could see the specifics - as with the death numbers and group populations in the 80 years and over category - then the conclusion would collapse. So they tried to hide things.
The tone and language of the study report implies that it would be for people in general. However, twice it is mentioned - restricting Hydroxychloroquine use “to well-selected COVID-19 patients” and that the study supports the claim that the low-dose regimen “is not associated with increased short term risk of cardiotoxicity and mortality in the hospital setting and in well-selected COVID-19 patients.”
Okay, so it really isn’t true for people in general, only “well-selected” patients. And that it might be beneficial not compared to other, safer drugs, but to no other drugs at all, which isn’t really the question.
Leaving out the death figures and percentages for the age groups is crazy. I looked at the extra stuff at the end right before the references, where it says, " Appendix. Supplementary materials." No help there…
No “miracle cures,” as we’ve noted. Steroids/corticosteroids/glucocorticoids do make a substantial difference, but mainly when a ventilator is in use and/or supplemental oxygen is being given (so I guess this means that things are pretty darn bad already).
Hydroxychloroquine does show some beneficial effect in making symptoms lessen and go away. What holds it back is the number of adverse events - Covid-19 is harmful, often, to quite a few organs, and a drug that presents increased risk itself of harm to organs is going to have a tough time being accepted.

 I don’t know - something does not seem to be right.
I don’t know - something does not seem to be right.
 And that it might be beneficial not compared to other, safer drugs, but to no other drugs at all, which isn’t really the question.
And that it might be beneficial not compared to other, safer drugs, but to no other drugs at all, which isn’t really the question.