This is a paradox. I like paradoxes. They tell us where our dogmas is wrong. The french paradox was that people who eat the most saturated fat got the least heart disease. That was a sign that our dogma that Saturated fat caused Heart disease was wrong.
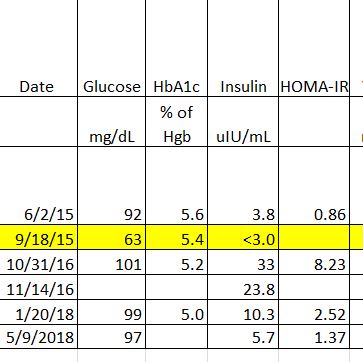
Let’s look at just one signal, Insulin. Some of us make a lot, some of us make a little.
Insulin promotes the transcription of DNA into mRNA to make the enzyme Acetyl-CoA carboxylase (ACC) 4x. Insulin also promotes the transcoding of mRNA in our cells into ACC up to 30x via sterol response element binding protein (SREBP)-1c.
Insulin also puts energy into the ACC enzyme by phosporylating it so it can do it’s job faster. As does glucagon which in T2DMs is inadequately inhibited by insulin.
OK so what does having more ACC that has been primed for action mean?
ACC is an enzyme that potentiates the conversion of Acetyl-CoA (from any source) into Malonyl-CoA - the rate limiting enzyme for cross-converting generic fuel into storable fuel (De novo lipogenesis). Even if you have no carbs in your pipeline, if you have more insulin you will be making more Malonyl-CoA although this study focused on glucose as a driver for insulin.
Normally ACC is stimulated by signals of energy excess, namely citrate in the cytosol (a signal of ATP sufficiency) and inhibited by PalmitoylCoA which signals an excess of fatty acids. However insulin apparently drives ACC independent of those.
OK so ⇈ Insulin ⇨ ⇈ Malonyl-CoA
What does that mean?
Well Malonyl-CoA allosterically inhibits the high speed transports (Carnitine Palmitoyl Transferase enzyme embedded into the membrane of the mitochondria) that bring fatty acids longer than 16 carbons long into your mitochondria to be used for energy.
https://www.jci.org/articles/view/15715
That inhibition in a hyperinsulinaemic type 2 diabetic was found (in rats) to be over 50x of that of a non diabetic.
Those fatty acids in an obese T2DM are the primary source of stored energy. That is the fat we make when we have too much energy. It is also the primary fatty acid that we store in our body fat.
To be used they have to follow a slower, more heat and peroxide (ROS) generating pathway through the peroxisomes to be cleaved into MCFAs and SCFAs that can then diffuse passively into the mitochondria.
That is why they await processing pooled in lipid droplets in cells. Those intramyocellular lipid droplets are a marker for insulin resistance in the greatest glucose sink thus driving further hyperinsulinaemia. It is also why in frank T2DMs triglycerides and NEFAs are parked unable to be used in circulation.
Remove the high insulin and now fuel is more efficiently turned into energy, and your AMPK signals to your body that you have lots of energy, and now satiety happens earlier.
Think of it like a hand basin. If the drain is open you have to run the faucet at full for a long time to come close to overflowing the hand basin. However let’s say the drain is partially clogged by hair in the drain. Then even a small flow from the faucet could overflow that basin.

Pull out that clog and the sink empties at a rate that is mostly independent of the faucet refill rate.
The water going down the drain in this metaphor is the process of turning fuel into energy, it is our mitochondria turning glucose, fatty acids, or protein into ATP. The faucet is taking in more or less fuel as food. The overflowing basin is stored fuel - body fat. And of course the hair clog is insulin inhibiting getting fuel into your engine.
For such a person limiting non-caloric nutrients to essential requirements and eating a source of energy that does not clog the hand basin means that energy freely flows from source (storage and intake) to sink (muscle cells being the largest sink). Satiety signals are driven in part by the conversion of fuel to energy (incl: AMPK).
In other words a person eating to satiety will eat less. The faucet is coupled to the drain throughput. The more energy is being generated (water flowing through the drain) the less food intake is required (water from the faucet). As the creation of energy drops (the flow through the drain drops) satiety signals cue the intake of more fuel (turn up the faucet).
That is why “Fat to Satiety” works to reduce the insulin demand in over 90% of participants on the Virta study and reverse the diabetes of over 60% of subjects in 1 year. And as a nice side effect, it additionally reduces their stored energy (body fat) for self evident reasons. Prof Phinney and Dr Hallberg pulled the clog out of their hand basin and their faucets turned down while the basin emptied and then once the basin was empty the faucet turned back up again.
This is also why the Ebberling/Ludwig 2018 paper showed that for every step reduction of carbohydrate intake the metabolic rate rose. It Dr Ludwigs subjects some had no blockage, some had some a slight blockage in the drain, and some had dropped a hand washer in the sink stopping most of the flow and he was able to observe that depending on what was in the drain changed the rate that water flowed through the drain.
It is also why Kevin Halls Met. Ward studies using isocaloric feeding don’t show an advantage because in Kevin Halls hand basin when you turn down the faucet to a hypocaloric drip, every sink empties. Calories in Calories out, FTW!