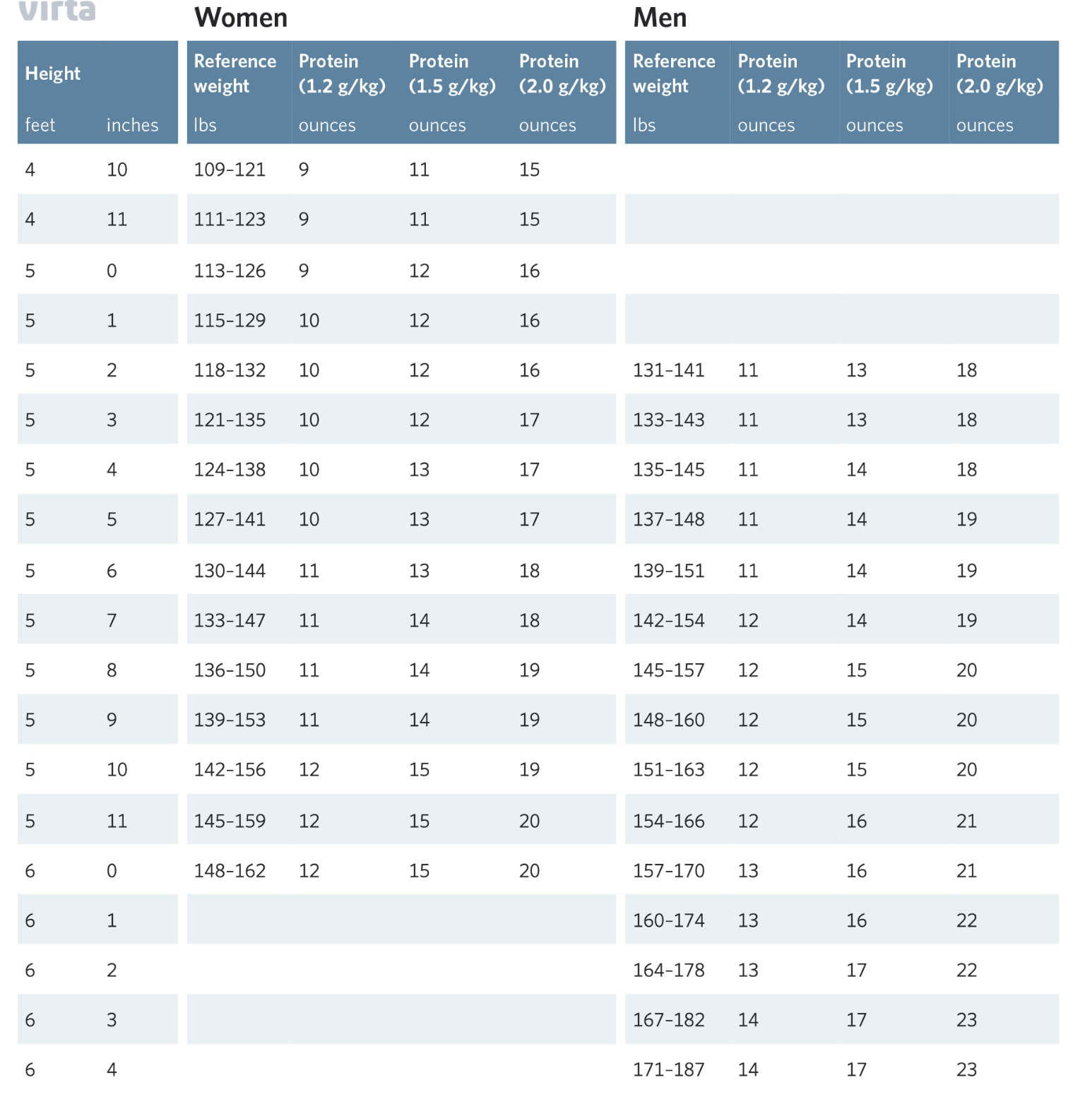
This is a really interesting article on protein and has a great chart about how much meat per height for men and women is in the ratio for protein in oz consumed.
Recently I haven’t tracked macros, but some days, mentally, it seems like I’m overconsuming protein. According to this chart, I am not overconsuming protein. This especially on 2 meal a day days and OMAD.
Preventing sarcopenia is really important to me at 65yo. My gym workout is helping me build muscle (that I can see in visually and in strength) so I’m guessing that I’m at the right ratio for me also given I am able, currently, to lose 1.5 to 1.9 lbs a week doing one EF a week.
My dermatologist is surprised that I don’t have loose skin. I guess I am getting some autophagy when I fast even if my GKI ration is >2 most fasts.
[1] “…A well-formulated ketogenic diet, besides limiting carbohydrates, also limits protein intake moderately to less than 1g/lb body weight, unless individuals are performing heavy exercise involving weight training when the protein intake can be increased to 1.5g/lb body weight. This is to prevent the endogenous production of glucose in the body via gluconeogenesis. However, it does not restrict fat or overall daily calories. …” …More
[3] Preventing sarcopenia? Dairy and Its Effect on Insulin Secretion (and What It Means for Your Waistline): “…I think it’s more accurate to say that acute insulin spikes are different from chronically elevated insulin levels, especially when it comes to appetite regulation and metabolic derangement. Consider this study, whose authors gave either whey protein isolate or whey protein hydrolysate to subjects 30 minutes before a pizza meal. Subjects given whey protein isolate, but not whey protein hydrolysate, reduced post meal blood glucose and insulin levels, and ate less pizza. The whey still released insulin, but it didn’t linger for very long and it led to improved post meal numbers. It wasn’t chronically elevated. The subjects weren’t hungrier, contrary to what you might expect from someone who’d just experienced a jump in insulin. …”
daddyoh
(Eric - The patient needs to be patient!)
#3
Using body weight as a referenced would have me eating a lot more protein. I think most days I eat 12 to 16 oz of a meat or eggs. Plus I get some protein from other sources when I have them like cheese, pork rings etc.
There seems to be a lot of variance in remediations out there. I listen to my body and watch my muscle strength and visual growth.
They are using total body weight? Most recommendations and studies are based on lean body mass which makes more sense to me. The extra weight someone carries as fat isnt going to require any protein, in fact losing the supporting tissue can be a source of protein.
As far as individual protein intake, all you need is to remain in ketosis, if you need the ketones, and not to exceed your body’s ability to rid itself of nitrogen metabolized into ammonia etc.
Richard has a great video about the natural variation of protein amounts in humans.
Examining research, theories, and efficacy are not “ADVICE” my dear?
Please explain what the “context” of a well formulated ketogenic diet really is so we can have your “official” understanding and approval about what makes sense to you so you can readily give “advice” to the world?
Right now I’m confused?
I don’t recall seeing a rule book of this “context” posted anywhere on the forum about what works and what does not on a ketogenic diet as Richard posted on an earlier thread “we don’t care how you get their?”
Now if you are talking extremely high levels of protein (per meal) then I can see your point if your diabetic?
Abstract BACKGROUND: Patients with acute renal failure are in substantial negative nitrogen balance as a result of their extremely high protein catabolic rates. We prospectively evaluated a series of patients with acute renal failure managed with continuous venovenous hemofiltration to determine which nutritional and nonnutritional variables might influence protein catabolism and nitrogen balance. …More
daddyoh
(Eric - The patient needs to be patient!)
#7
No the table is driven off of height and has what Dr. Phinney calls reference body weight as a reference to his other recommendations for protein per reference body weight.
Sorry for referring to all of what you linked as “advice”. I’m saying one of the sources you’re using (Optimizing Nutrition) has made some logical errors. And while I appreciate some people can eat pizza and see be in ketosis, they would be the exception to the norm. Yes, I am biased toward the IR population also… [which it turns out is exactly what daddyoh is dealing with.]
I am using studies and biochemistry as linked and explained by people much smarter and well referenced than myself, but I do understand the basics.
As to “context”, the state of ketosis changes the fundamental way protein influences insulin, glucose and glucagon in the body so there is a big difference between a low carb approach while not in ketosis and a ketogenic approach. There is nothing wrong with low carb. Since this is a ketogenic forum, however, I think it’s important to point out the differences. I’ll spare us all another Bikman video here.
daddyoh
(Eric - The patient needs to be patient!)
#10
That did not work for me. I have to guard my carb count so closely. I deviate for Mexican refried beans measure in a couple of tablespoons.
Lately, I have drifted toward carnivore but I’m not there yet. My fasting is easier, my feasting has me fuller earlier and my weight loss rate is going up.
You have to love Bikman. I learn so much from him and he calls it as the evidence shows us.
daddyoh
(Eric - The patient needs to be patient!)
#11
Dr. Phinney explains there are problems with people interpreting idea body weight so I think they named it reference body weight. I’m not sure if they line up. I’m just using my height in the table.
And no I’m not talking about renal failure or damage. I’m talking about 1) remaining in ketosis, esp if IR and 2) ammonia toxicity if ingesting over around 3.2 g/kg/lbm. Thise would be the limiting factors on the high side. On the low side would be adequate protein for a positive nitrogen balance based on individual biology and exercise. Richard references all the appropriate studies in his youtube.
”…While it’s probably not wise to go hog-wild with protein supplements and powders if you have diabetes, swinging to the other extreme to target minimal protein levels is a sure way to end up with a poor nutritional outcome.
According to Simpson and Raubenheimer in Obesity: the protein leverage hypothesis (2005), people with diabetes may actually need to eat more protein to ensure that they have adequate amounts to build lean muscle mass given that higher levels of gluconeogenesis may cause more protein loss to glucose due to their insulin resistance.
”…One source of protein loss is hepatic gluconeogenesis, whereby amino acids are used to produce glucose. This is inhibited by insulin, as is the breakdown of muscle proteins to release amino acids, and therefore occurs mainly during periods of fasting (or low carb).
However, inhibition of gluconeogenesis and protein catabolism is impaired when insulin release is abnormal, insulin resistance occurs, or when circulating levels of free fatty acids in the blood are high. These are interdependent conditions that are associated with overweight and obesity, and are especially pronounced in type 2 diabetes (12,34).
It might be predicted that the result of higher rates of hepatic gluconeogenesis will be an INCREASED requirement for protein in the diet. …” …More
Advising someone who is insulin resistant to create more endogenous insulin than necessary is counter-productive in the long term goal of healing that resistance and liberating bodyfat. In a non-keto diabetic, replacing carbs with protein will be benefical. If someone had borderline T1D, or super low insulin then combating blood glucose excursions via inhibiting FFA release with insulogenic foods makes more sense.
IR a spectrum. At the beginning you will see an increased post-prandial insulin response to glucose, which is a warning sign of things to come. Unfortunately, the test for this is only ever performed as a normal standard of care during pregnancy to detect gestational diabetes.
The next phase is where elevated insulin is increased after a meal but glucose cannot be contained, this phase can coincide with an increased basal insulin. Final stage is loss of or diminished pancreatic function - then adding insulin is required, but less so if managed by VLC diet. https://www.diabetesresearchclinicalpractice.com/article/S0168-8227(16)30157-7/fulltext
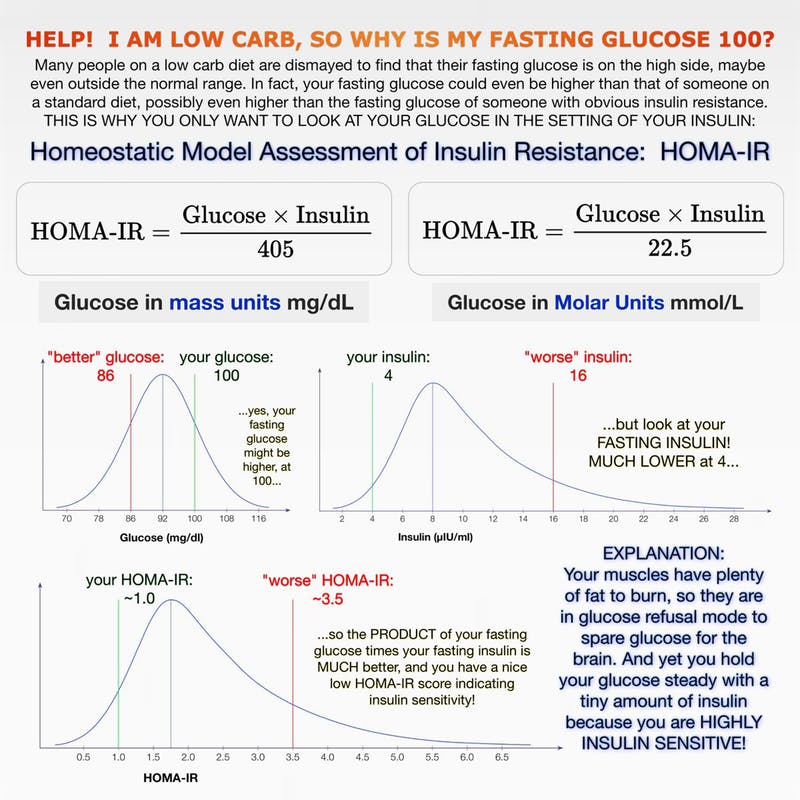
”…As Dr. Naiman recently posted, only testing fasting blood glucose without testing fasting insulin tells you very little. That’s because two people could have exactly that same fasting blood glucose levels and have very different circulating insulin levels.
It is all about the relationship between glucose and insulin and how they work in concert. This is called the homeostatic model assessment of insulin resistance or HOMA-IR. The name is a mouthful, but it simply means that the body is always trying to keep its essential systems in balance or in an equilibrium — called homeostasis. Insulin is working against glucose in an attempt to keep blood sugar levels stable, a.k.a in homeostasis.
In one individual — for example someone with pre-diabetes, type 2 diabetes, or polycystic ovarian syndrome — insulin may over time be pulsed out in higher and higher amounts just to keep the blood sugar relatively stable. While fasting blood glucose could still be in the normal range, it is taking increasing amounts of insulin to keep it there. As insulin resistance develops, and insulin becomes increasingly ineffective to bring blood sugars down, blood sugars will eventually rise too high.
In a second individual — someone who has been on the keto diet for a number of months and is now burning fat for energy — only tiny amounts of insulin are being pulsed by the pancreas to keep the glucose stable. You are now, therefore, no longer insulin resistant, but very insulin sensitive and only need small amounts of insulin to keep glucose in check.
Dr. Naiman’s graph shows, if you know your fasting blood glucose and your fasting insulin, the HOMA-IR equation can tell you how insulin sensitive or insulin resistant you are. If your fasting blood sugar is 5.7 (103) and your insulin is high, too, over 12 μU/mL, you are insulin resistant and on your way to type 2 diabetes. If your blood sugar is 5.7 but your fasting insulin is under 9 μU/mL, you are insulin sensitive and likely in glucose refusal mode from a low-carb diet.
Most doctors do not yet check for fasting insulin with a fasting blood glucose test. You usually have to ask for it. …” …More
Yes, that’s a great start based on easily available testing. But there are raised post-prandial levels before a HOMA-IR will show much. Here’s a podcast and summary of other methods to measure IR and how they stack up to the “gold standard” of the insulin clamp.
…the “ best overall predictorsof insulin resistance were theMcAuley, Matsuda and Insulin AUC, which were essentially identical in predictive performance ”
When your talking from that aspect Chris Kresser pretty much hits the nail on the head, although not an exact science, he has a good grip on the reigns of this?