
Been into Keto since Halloween 2024. Have lost about 35 pounds (should’ve weighed myself right at the start, but didn’t), down from about 230 to 195. I am a 5’-10" 62 y/o male. BP is down and I feel great. I have had high ldl cholesterol for years (hdl has been going up since on Keto and Triglycerides are good) and was actually on statins for a year or two probably tens years ago. Stopped taking the drug because it noticeably increased joint pain in my knees, ankles, and shoulders. I had multiple injuries to those joints over the years, from both sports and work related. Also, the surgeon who recently repaired my shoulder, as well as an ortho that I saw for a sudden short flareup of severe ankle swelling and pain, have both informed me that I have osteoarthritis. However, the joint pain is much less severe without statins.
Went to my General Practitioner in March, I’ve only been seeing him for a couple of years. Prior to that I went years without one. Since my first visit he has been on me about my ldl and during the last visit he recommended statins. I told him about my prior experience with statins so we agreed that I should get a CT Coronary Artery Test, also known as a Calcium Score. Had the test today and just reviewed the results online. My total calcium score was through the roof. Total Calcium Score = 2327. I realize that this test only identifies your RISK for heart disease, not the presence of it. But, that is a really high score as they say over 400 is “high risk”. I’ve had two discussions with my doctor about ldl cholesterol and the research which maintains it is not really a valid marker for risk of heart disease. He however, is still in the “reduce fat, reduce cholesterol” camp.
The results of the test will be automatically forwarded to my doctor. I know that he is going to want to put me on statins and get on a low-fat diet. That is not going to happen. Just wondering if any of you have further info on ldl cholesterol studies or your personal experiences with high ldl cholesterol as well as high Calcium Scores?
Very High Calcium Score
Start here. You can work forward or backwards from here. As my cardiologist said there is not a single study (RCT) that showed a statin is more effective in treating heart disease over a well formulated ketogenic diet.
There’s a lot of info concerning CAC scores (the good, the bad, the nuanced) on the forum. Search around and follow some threads.
Short answer: Calcification in arteries is actually the healing of soft plaque - which is the dangerous initial stage which can come loose and wreak havoc. Calcification represents “scabbing” and stabilizing the soft plaque - it’s also the only kind that shows up (i.e., is echolucent) on a CT scan used for CAC calculations.
Yes, your Agatston CAC score is high. It’s likely to reflect attempts your body is making to heal decades of prior soft plaque damage from inflammation.
Statins will NOT help anything that you’ve shared about your health issues. Period.
Some reading material below (highlights provided for convenience)

Statins-LowCarb-Aug22.pdf (552.9 KB)
StatinAdherence-CVD.pdf (413.4 KB)
High Coronary Calcium (CT) test score
My research on this topic (done some time ago) suggested that however high your calcium score, your most important marker to measure is your increase in calcium. If you can arrest the increase in the score, you minimise the cardiac event risk.
How do you do that? I remember listening/viewing some podcasts/YT vids of people that had reduced their high calcium score (admittedly not by much, but IMHO reducing the calcium is the healthiest thing you can do). In general, the strategy was to minimise inflammation, and that meant as low carb a diet as possible. I am pretty sure that one of those vids was with Ivor Cummins.
Personally, if I had that high a CAC score (mine was actually 10 with a current LDL level of 450!) I would go strict carnivore, do some serious meditation, and do some exercise every day. I would never take a statin. Poison.
The only qualifier I’d add is that the calcium reflects only hard plaque which is the healing of non-echolucent soft plaque - which is the danger if it comes loose.
As such, while no (soft) plaque is best, the calcified plaque (which is echolucent and shows up on a CT scan) is evidence of previously soft plaque that has since been immobilized.
And so things are more nuanced than simply saying that “no plaque” is best given the difference in which stage of plaque is dangerous and which shows up on a CAC test.
Hope this isn’t too fine a point on things.
Thanks to Mark, Alec, & Joey for the replies. Been doing a little research on the whole Calcium Score thing. It is well known that the test does not identify arterial blockages, it is supposedly predictive of the risk of same. Another aspect that I find interesting is that the test only costs about $50 because it is not usually covered by insurance. Other tests done with expensive medical equipment like the CT Scanner are extremely expensive. So, are those other tests obscenely overpriced because they are covered by insurance and we all wind up footing the bill via higher premiums and co-pays, or is this just a case of the medical profession being charitable? Ha Ha Ha, fat chance of that!
My guess is that those other tests are way overpriced but that there is an ulterior motive for the Calcium Score testing to be provided for such a relatively low cost. You can probably see where I’m going with this. It seems to me, that this test was devised by big pharmaceutical companies (around 1990) to get people to comply with their minion’s (doctor’s) orders to take statins. I’m guessing that not getting the huge profit margin that they do for other tests must be more than made up for in the increase in the volume of statins they can push to the general public.
Thanks to Mark, Alec, & Joey for the replies. Been doing a little research on the whole Calcium Score thing. It is well known that the test does not identify arterial blockages, it is supposedly predictive of the risk of same. Another aspect that I find interesting is that the test only costs about $50 because it is not usually covered by insurance. Other tests done with expensive medical equipment like the CT Scanner are extremely expensive. So, are those other tests obscenely overpriced because they are covered by insurance and we all wind up footing the bill via higher premiums and co-pays, or is this just a case of the medical profession being charitable? Ha Ha Ha, fat chance of that!
My guess is that those other tests are way overpriced but that there is an ulterior motive for the Calcium Score testing to be provided for such a relatively low cost. You can probably see where I’m going with this. It seems to me, that this test was devised by big pharmaceutical companies (around 1990) to get people to comply with their minion’s (doctor’s) orders to take statins. I’m guessing that not getting the huge profit margin that they do for other tests must be more than made up for in the increase in the volume of statins they can push to the general public.
The CAC scan is cheap because it is. It is about $100-$300 for me. The other tests require other things like an injection and higher quality scans. It may also be reading it too.
The CAC score is beginning to get used to STOP statins. So, if you have a score of zero, some docs (not all, of course) will not prescribe statins. My new cardiologist, younger, saw my zero score and said he wouldn’t prescribe statins, even though my LDL is over the (ridiculously low) limit of 100.
Like this, for instance:
https://academic.oup.com/eurheartj/article/41/Supplement_2/ehaa946.2923/6004698?login=false
@Brian_O Great question…
Our annual his and her CAC scans cost us $69 (out of pocket - not covered by insurance). No price increase over past 5-6 years. We then get a follow-up call from the hospital’s affiliated cardiologist to make an appointment (no thanks).
As @ctviggen notes, it’s cheap because the marginal incremental cost of running an incredibly expensive machine is small. While the opportunity for the hospital to up-sell medical services is high.
It’s a very straightforward business model. The Agatston CAC score is a starting point. It’s volume-oriented. If you take the calcium mass and divide it by the calcium volume you get calcium density. That’s not in the score - but the full report provides this vital info.
Calculate your density over time - higher density means the scabs are working their magic and protecting against what could have been previously life-threatening soft plaque.
This is all far too complicated to explain in marketing materials. Then again, what does one expect for $69 bucks?
@kib1 EDIT: Sorry, should have posted these …
CalcDensityPlaque-Criqui-2017.pdf (508.4 KB)
CalcDensityPlaque-Criqui-2014.pdf (323.7 KB)
Are they seriously targeting this now??? That is crazy…. Dangerously low. The pharma industry has NO morals. They care for one thing: their profit level.
My Dr prescribed a CT angiogram (ie the more expensive one) that also sees soft plaque. It cost me around A$300, which is approx US$200. To me, not expensive to see what might or might not kill me!
- See Ben Bikman’s Metabolic Classroom posted yesterday, re nattokinase and it’s possible use in lieu of statins.
BTW, Bikman is kinda down on LDL, too, so maybe some comfort, or better measures, like triglyceride to HDL ratio.
- I’m 68 and my CACS score is 1200+, so I hear you. That scan doesn’t see hot necrotic about-to-kill-you placque, only healed over scars (the calcium). But not all calcium is atherosclerotic. Some people develop calcification because Vascular Smooth Muscle cells are not terminally differentiated --they can divide and grow. Bad ju ju like diabetes or hepato-renal syndrome can make VSMCells morph to become like osteoblasts (bone making cells). Perhaps a more sophisticated test can help. Matt Kaberlein recently did an Optispan podcast about his recent “Clearly” screening, an AI-enhanced angiogram that can discern intimal vs medial calcification.
 … That could explain a lot! What a game changer, if it’s actually the VSMC’s that are creating the deposits in some cases.
… That could explain a lot! What a game changer, if it’s actually the VSMC’s that are creating the deposits in some cases.
This is from one of my tests (which I paid for myself):
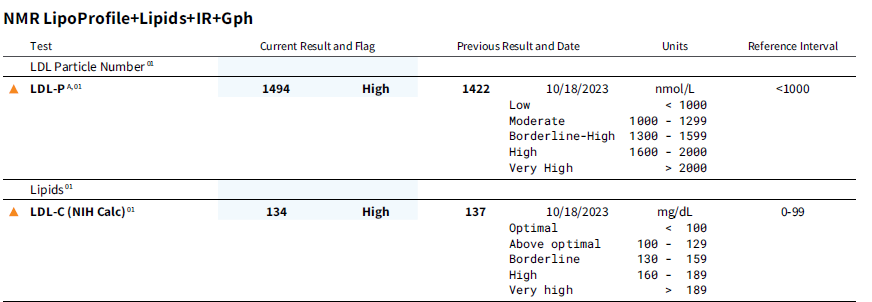
The bummer for me was/is that my HDL is dropping into the mid 40s from low to mid 50s and trigs are slightly above 100, when they were closer to HDL. Can’t figure out why.
Bob
IMHO, if you are not eating carbs, then you need not worry about where your HDL or trigs are. They are where they are supposed to be. Trust your body if you are feeding it the right stuff. But if carbs are creeping in, maybe it’s a sign?
Cheers
Alec
I do not have particularly high cholesterol. My last test this last December was around 175 LDL-C. My LDL:HDL ratio was 2:1. I was doing keto with some fiber, and my blood ketones were 1. My blood pressure is way down from 4 years ago at the 100s/70s range and sometimes lower. I have never had a CAC test or other specific test for CVD, but suspect I managed to give myself some a few years back. I second the opinion that the reason your CAC is so high could be that going on Keto gave your arteries a chance to start healing - which involves becoming calcified… Calcified plaque is better or “more stable” than “hot” or actively growing plaque, which is more likely to rupture, form a blood clot, which can give you a heart attack, stroke, etc. But, again the CAC test is not terribly specific when it comes to CVD. I would at least do a carotid artery ultrasound, which will show the degree of active plaque in your carotid arteries. You could follow it up in some months to see if it is worsening or getting better.
I too do not like the idea of statins, and never plan to go on any for the purpose of reducing cholesterol. However, there are some studies which show some statins tend to squelch the inflammation in the arteries even at low doses… a small dose 2-3 times/wk. That can also give the arteries time to heal. If I had raging CVD, I probably would consider this to help the healing process. Nevertheless, there is no pill that is going to overcome the consequences of a poor diet ie the SAD on a daily basis. So doing keto is more important to healing than a drug, IMHO. I also recommend getting yourself an oxLDL test or a PLAC test, which will give you an idea of the amount of oxidation going on with your LDL, which I believe is a main driver of CVD. Ideally, you want oxLDL <60. You can get this yourself throuqh Quest Labs. Since you are doing Keto, you can expect a decent score.
Thanks for the info. My ldl is 209 and hdl is 71. Triglycerides are 66 for a 0.9296 to 1 ration of hdl to triglycerides. Feeling great, BP is down. Thought for sure I’d be hearing from my GP about the high calcium score but apparently he’s not concerned, lol. As far as I can tell I’m doing all I can. Probably not going to get any more tests.
I have always had high cholersterol (with high HDL) but refused to take statins.
Not overweight, no diabetes and doing sports 6 days a week.
I was already eating low carb, but drinking wine and snacking crisps almost every day.
Three years ago , I was 66 yo then) my GP forcedme to do a calcium score test.
Result was 4335…
Started statines but they made me feel miserable.
Than came Praluent + Ezemtimibe , still felt miserable and cholesterol stayed high.
Next step Repatha + Ezemtimibe my LDL went down LDL is now 2,77 , HDL 2,54 , trigycerids 0,75 (all mmol/liter)
My doctor is happy but I feel like ■■■■■ sore muscles esp my legs, headaches, brainfog, stress!
Started Keto 2 weeks ago , within a week my feet were not swollen anymore!
My next Repatha jab is due tomorrow, don’t know what to do???
@Sjaak Welcome to the forum!
Wish I had some meaningful info to share based on what you’ve posted above. But lacking this, I’ll share some articles that might be of interest as you navigate the “statin vs no statin” terrain. Food for thought…
StatinAdherence-CVD.pdf (413.4 KB)
Statins-StatisticalDeception-Diamon-Ravnskov.pdf (578.0 KB)
StatinTherapy_CAC_Effects.pdf (221.7 KB)
Thanks it seems I might as well stop lowering my LDL…
I suppose Praluent and Repatha are doing the same thing so I am seriously considering to stop taking Repatha.
Taking drugs to lower cholesterol is no longer regarded by many practitioners as good science. Cholesterol is not bad. Nor is it deemed to be a diet-induced thing. Our own bodies produce it and our brains are composed of roughly one-half cholesterol.
Not your doctor here, of course, but… the 1980s called and wants their science back.