Thanks all for the ideas, here are some responses. I feel like if I can troubleshoot my issues, it might actually be really helpful to others who are experiencing similar long-term LCHF issues:
I’ve done this before but good idea.
True, though I am quite certain I’m as low carb as I was before. Nevertheless, a food diary isn’t a bad idea.
Frankly one hypothesis I have is that my metabolic rate has dropped as a result of eating low carb for so many years. No evidence to back it up though.
I’m concerned about both ALT and AST. Even when they’ve both been in the early 20s, they’re a worry. Peter Attia likes his patients to have them in the low teens.
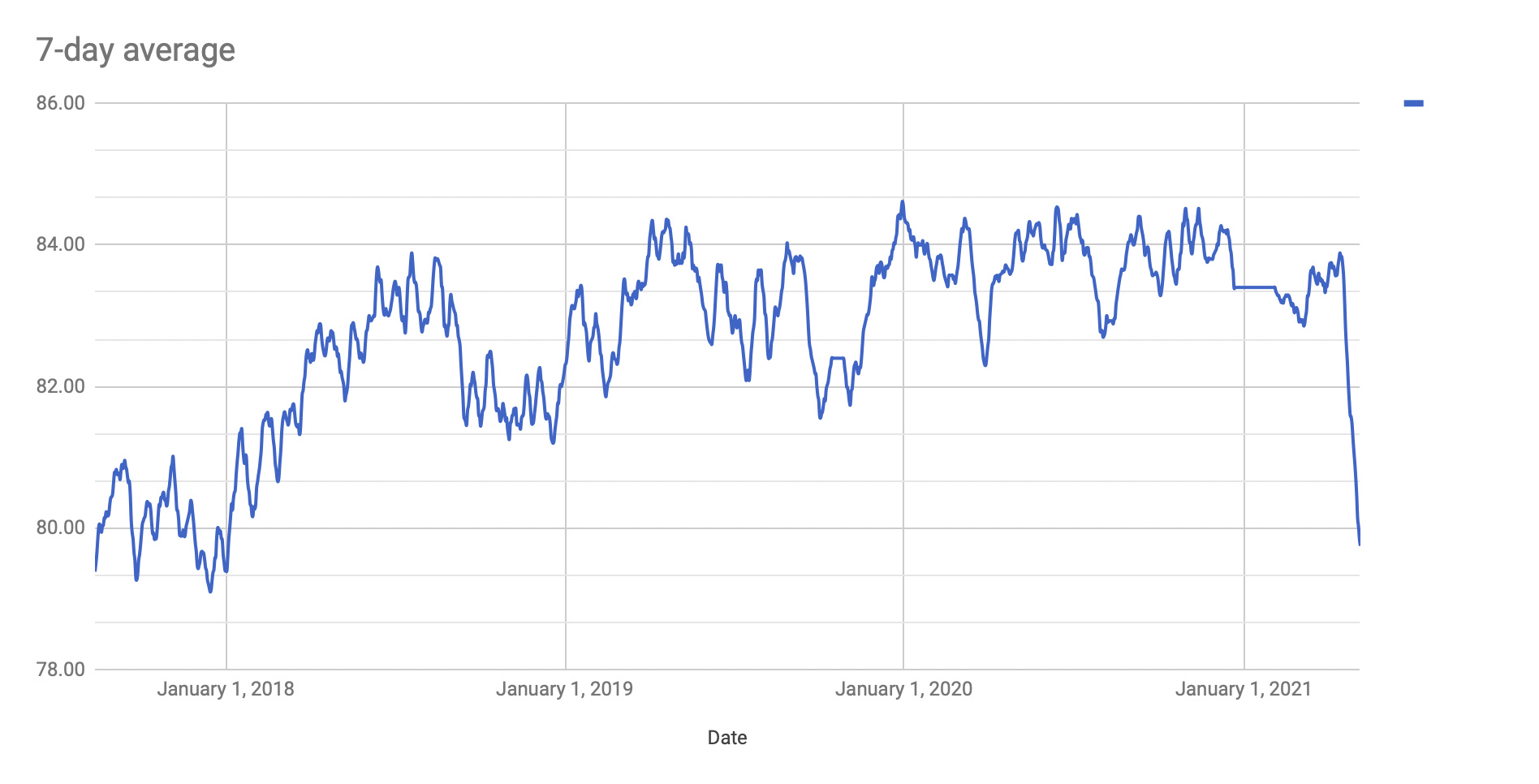
No, I’ve become more and more sedentary during covid and if anything lost LBM. Though I think I will need to add exercise (especially strength training), I don’t see a correlation between the weight gain and exercise. I was getting loads of steps in every day in NYC, and doing single set to failure strength training, and was trapped in the 82.5-83.5kg range for a long time.
The thing is, when I was wearing a Freestyle Libre, I didn’t have high BG in the morning. CGMs aren’t very accurate in my experience, but I felt like generally my BG was optimal (80-90 in US terms) and stable.
Yes, kind of, and yes. Right now, I drink mostly cream cappuccinos, eat cheese, eat peanut butter, have almond flour stuff occasionally, and haven’t consciously dropped oils/butter. Could totally try all of this for a few weeks.
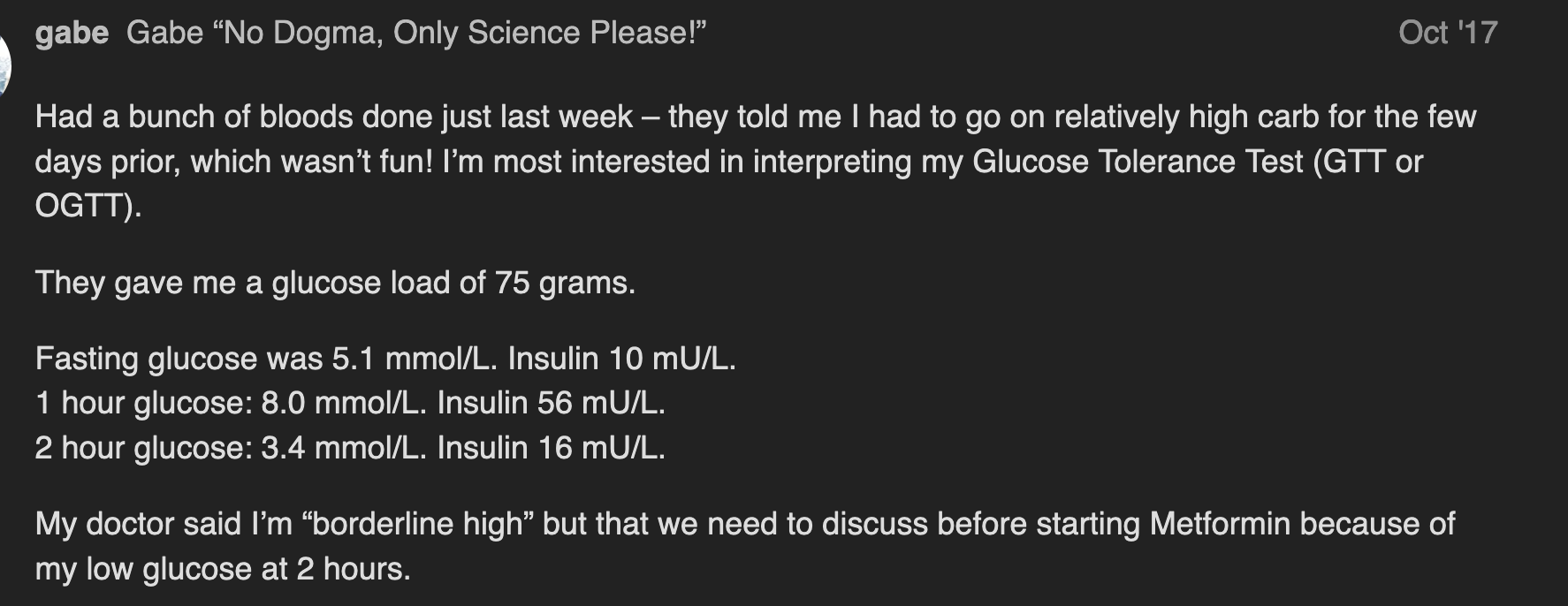
Yep, I actually went back and looked at the notes I took in my weight-tracking spreadsheet, and I wrote that I was having high carb prior to the OGTT. The results are in this post: https://www.ketogenicforums.com/t/help-me-interpret-my-glucose-tolerance-test/21061?u=gabe
Not massively different than usual. If anything less, on balance, than at my last job. So I don’t think it’s correlative with my weight gain/stall.
Rheumatologist said today that he’s determined that I don’t need him and he referred me to a sports doctor and an endocrinologist to help me resolve the mechanical joint issues + the weight issue. In fact he thinks I shouldn’t waste time with the latter and see if the sports doctors can help me solve the problem with training.
No meds.
When I cook, I use allulose, but it’s very expensive here in Australia. The chocolate I currently eat is made of stevia and erythritol. That could be a factor. Though I’ve gone zero sweetener before, and it hasn’t moved the needle…
I am super careful nowadays to avoid vegetable oils of any kind. I eat primarily butter and olive oil, with some coconut oil. The only veg oils I’d consume would be in delivery food, and I’ve been eating at home almost exclusively since March!
I’m back in Australia. While I’ve been much more sedentary, I spent all of winter in the sun and I’ve been getting out now in the spring – because we’ve almost eliminated the virus here, I now feel comfortable sitting at cafes etc.
Thank you Madeleine!
Thanks @PaulL, see above re OGTT. Paul Mason actually looked at my results at Ketofest in Canberra a couple of years ago and said, “yep, you’re insulin resistant.” I go a bit hypoglycemic after a 75g glucose load. My GP had said as much when I had the test in 2017. It’s not enough for them to insist on Metformin, but to give some context, the same GP who gave me the OGTT in 2017 recently prescribed me extended release Metformin at my request. I haven’t started taking it though because my sudden hearing loss in late 2017 came shortly after I took Metformin the first time – that latter half of 2017 was the first time I really started trying to troubleshoot the stubborn weight loss stall.
Anyway… I suspect there are no simple answers to any of this. I may have to do some trial and error with some of the suggestions people have made above. It may well be that my Phinney weight is just higher than I’d like, though from a mechanical perspective this wouldn’t be great in the very long term because of my joint (specifically knee) issues!