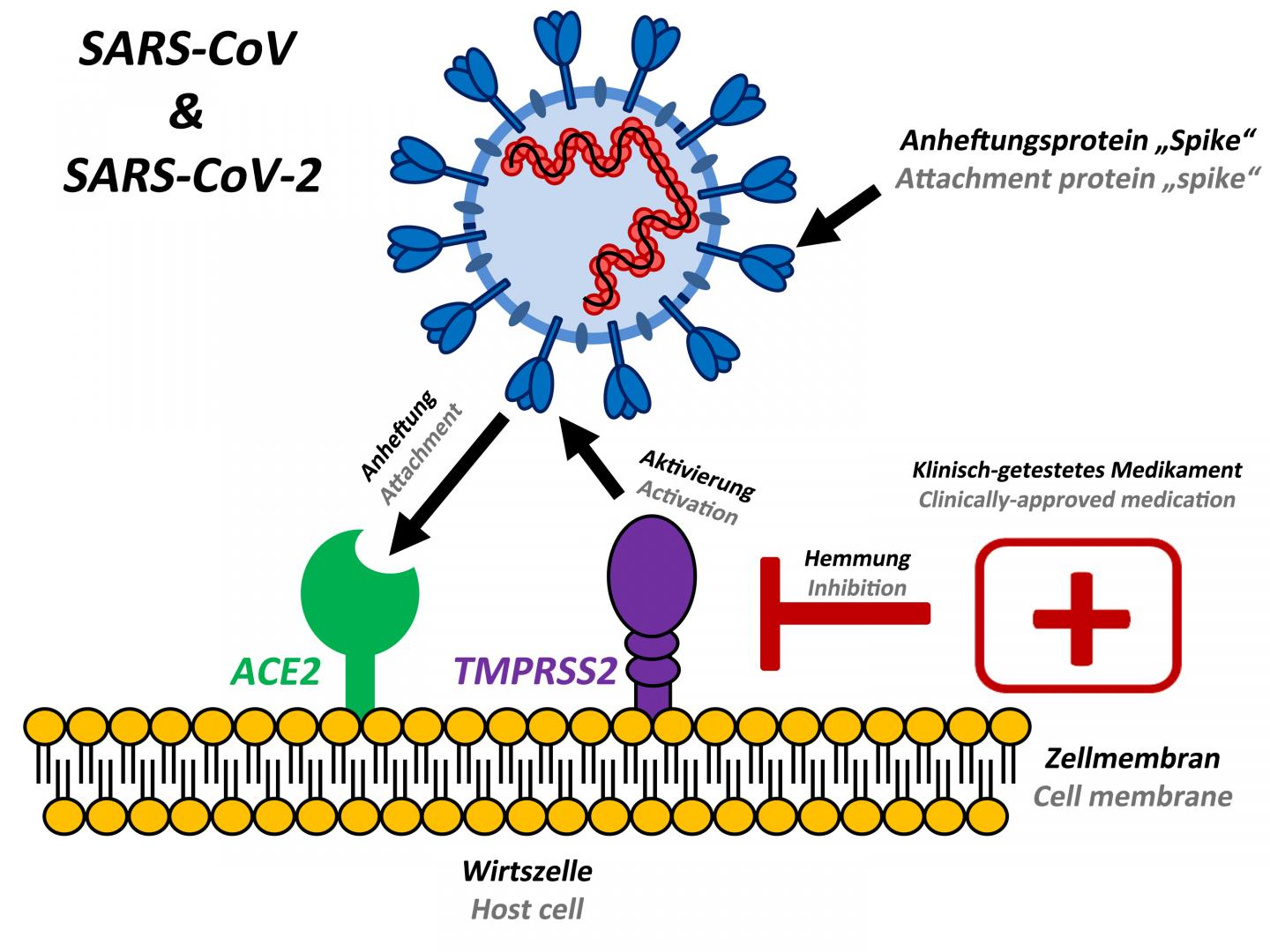
Agreed about ACE2, but the text does just say drugs “inhibit” the infection of lung cells - so that’s quite relative, i.e. how much do they really do that? It’s not like any such drugs are broadly effective or in use, from what I can see. It’s the “German Primate Center” - they may just be talking about lung cells cultured in a dish. That website specifies that for both SARS and the new coronavirus, “No vaccines or drugs are currently available to combat these viruses.”
The diagram doesn’t address the difference between SARS and the Covid-19 causing virus, which is, as far as I know, rooted in the spike proteins. It’s not shown on the diagram, but SARS-CoV-2 has a physically different spike - it attaches to human receptors in a smaller, more compact way, It’s a stronger attachment, and this allows more efficient infection of human cells - this is why the new SARS spreads faster than the old one.

 But all I see thus far is you guessing that a thing happens - that anti-A antibodies affect things. It was a thing with the first SARS, but is there any scientific proof that it operates with SARS 2?
But all I see thus far is you guessing that a thing happens - that anti-A antibodies affect things. It was a thing with the first SARS, but is there any scientific proof that it operates with SARS 2?