
Looking for some details on the science behind this medication- Mounjaro, particularly potential impacts for longer term. Realize it’s new, but looking for some input
T2 Medications Mounjaro
Rebj
(Rebecca )
#2
Welcome to the Forum. I’m sorry I can’t offer anything on the medication in question. Hopefully someone else can!
coopdawg
#3
I’ll welcome you by absolute default mate!
You need to provide us with more info tbh.
People won’t take you seriously otherwise.You do the work, and you will get considered opinions.
Hope to hear from you soon, right now I have no idea what you are requesting. 
skeptic888
(Bill)
#4
I presume you are talking about this…
Like all medications it will have side effects … better to change what you eat to avoid medication completely if at all possible (plus there are zero side effects to eating real food).
Naghite
(Michael)
#5
This drug lowers A1C by increasing insulin production. This is a very bad idea for any diabetic to raise insulin. Hard pass to everyone, no one should ever take this drug. It is not safe long term.
Shortstuff
(Allie)
#6
**Tell your healthcare provider if you get a lump or swelling in your neck, hoarseness, trouble swallowing, or shortness of breath. These may be symptoms of thyroid cancer. In studies with rats, Mounjaro and medicines that work like Mounjaro caused thyroid tumors, including thyroid cancer. It is not known if Mounjaro will cause thyroid tumors, or a type of thyroid cancer called medullary thyroid carcinoma (MTC) in people. **

Just the info on their website screams no…
TLC7319
(Tammy Cross)
#8
Thank you! This is exactly what I was looking for. Trying to understand the mechanism behind this medication. Much appreciated!
Auden
(Auden)
#9
I have the same question. The drug works really well in trials. If it does increase insulin, are we wrong about why keto works?
PaulL
(You've tried everything else; why not try bacon?)
#10
I’m not sure what you are driving at, but is increasing insulin secretion really a good treatment for a problem caused by insulin-resistance and hyperinsulinaemia? Especially since lowering the stimulus (namely, an excessive amount of dietary glucose—also known as carbohydrate) will automatically reduce the need for insulin? And also since a low-carb, high-fat, ketogenic diet has been shown to be effective in reversing Type II diabetes and insulin-resistance?
In any case, ketogenesis in the liver is stimulated by a low insulin/glucagon ratio. These two hormones work in tandem to regulate a number of processes in the body. Of particular interest to us is the production of ketones and glucose by the liver. When carbohydrate intake is low, the pancreas secretes glucagon to stimulate the production of endogenous glucose (gluconeogenesis) and ketone bodies (ketogenesis) to fuel various organs, including the brain. Insulin remains low because there is no excess of serum glucose to contend with. The resulting low ratio of insulin to glucagon signals the body to stay in fat-burning mode, and it allows fatty acids to leave adipose tissue to be metabolised, there being no need for glucose at that point, except by the cells that absolutely require it.
When carbohydrate intake is high, serum glucose rises, and the secretion of glucagon is inhibited. This allows insulin to signal muscles to start burning glucose instead of fatty acids, signal the liver to stop making glucose and ketones (since we want to metabolise the excess of glucose in the blood instead), and signals the adipose tissue to store fat and not release it. (Think of a bear eating lots of berries to prepare for hibernation; the body doesn’t want to be using up all that glucose, it wants to be storing it for winter. It’s not the body’s fault that we now have access to sweet foods year-round and not only in autumn.)
As carbohydrate intake remains chronically high, the cells that are forced by insulin to deal with the excess of glucose down-regulate their insulin receptors in self-defence. This is insulin-resistance.
It requires the secretion of ever larger amounts of insulin in order to force the cells in question to do their jobs. This results in hyperinsulinaemia. After some time, the cells can no longer cope with the onslaught of glucose, and the body’s glucose control starts to fail, since no amount of insulin is able to force the cells to take in more glucose. This is Type II diabetes. So you can see why I question the idea that forcing the pancreas to secrete even more insulin is an effective treatment, especially given that hyperinsulinaemia is damaging to many areas of the body.
Auden
(Auden)
#11
Thank you for replying! I’m actually not driving at anything. I’m puzzled that these drugs are working so well for weight loss since they raise insulin. How can this be possible?
I’m not too hardcore on the science these days, but the drugs mimic glucagon-like peptide 1 which I guess increases insulin. Maybe insulin isn’t as influential as we thought to weight loss?
Maybe high insulin is just another symptom of the problem (like the weight gain is). I remember being told my A1C was high because my weight was high, back before The Obesity Code came out.
But I’ve also read some things that they actually help with leptin. Maybe they overcome the insulin increase with some other mechanism like that.
Thanks for taking the time to explain how ketosis fuels the body.
Now that these insulin-raising drugs are coming out with weight loss labels, I’m wondering if a ketogenic diet might be fixing some other hormonal issue and the lower insulin is a side benefit, not actually how I’m losing weight (and NO, I’m not a CICO person at all). This is just speculation, but I’m remembering the days when they told you eating fat would make you fat and everyone thought Atkins was crazy, so I try to keep an open mind when things come along that challenge my world view and this study raising insulin and getting rapid weight loss makes me very curious.
PaulL
(You've tried everything else; why not try bacon?)
#12
Well, whatever these drugs do, it must be in spite of the higher insulin, not because of it. Insulin inhibits the action of hormone-sensitive lipase inside adipocytes, thus trapping triglycerides inside. An intact triglyceride is too large to pass through the cell wall; it must be broken down into its constituent fatty acids and glycerol in order to leave the adipocyte. It would be interesting to see a paper describing how such a drug can promote weight loss. Losing muscle mass and weakening bones would not be good means to that end.
ctviggen
(Bob M)
#13
This sounds like a recipe for disaster:
But the people taking the drug did lose weight. Their blood sugar decreased markedly. Did this cause them to be less hungry? Could it be that having a higher blood sugar = more hunger? Their fasting serum glucose (FSG) plummeted:
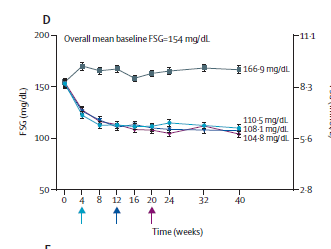
(There were three different levels of the drug given, that’s why there are three lines on the bottom, with the placebo on the top.)
Edit: Even they don’t know why people lost weight:
Naghite
(Michael)
#14
How does Mounjaro help with weight loss?
Mounjaro helps with weight loss by decreasing food intake and slowing down how fast food travels through your digestive tract (called gastric emptying). This may help you to feel fuller for a longer period of time and reduce how much food you eat. Studies show this action may occur in the brain.
- Mounjaro is a single molecule that activates glucose-dependent insulinotropic polypeptide (GIP) receptors and glucagon-like peptide-1 (GLP-1) receptors. GIP and GLP-1 are both natural incretin hormones.
- GIP has been shown to decrease how much you eat and increase your energy expenditure, which results in weight loss. When combined with a GLP-1 receptor agonist, this may result in greater positive effects on blood glucose and body weight.
- Mounjaro also slows the movement of food from the stomach into the small intestine. As a result, you may feel full more quickly and for a longer period of time, so you eat less.
Losing weight can improve how you respond to the insulin that your body releases from your pancreas, which helps lower your blood sugar.
PaulL
(You've tried everything else; why not try bacon?)
#15
I don’t think that works under a high dietary carbohydrate load, does it?
Naghite
(Michael)
#16
The quote was directly from the link I posted as with the rest of the text. I did not write it, nor am I claiming it is correct, simply providing a link to their explanation. While I am sure weight loss has some effect on IR, I personally do not think that is the only mechanism.
PaulL
(You've tried everything else; why not try bacon?)
#17
Or, possibly, it’s lowering insulin-resistance that allows fat loss to occur (since it’s hyperinsulinaemia that inhibits fat loss, and hyperinsulinaemia always accompanies insulin resistance).
ctviggen
(Bob M)
#18
They state the following:
Citation 14 is this one:
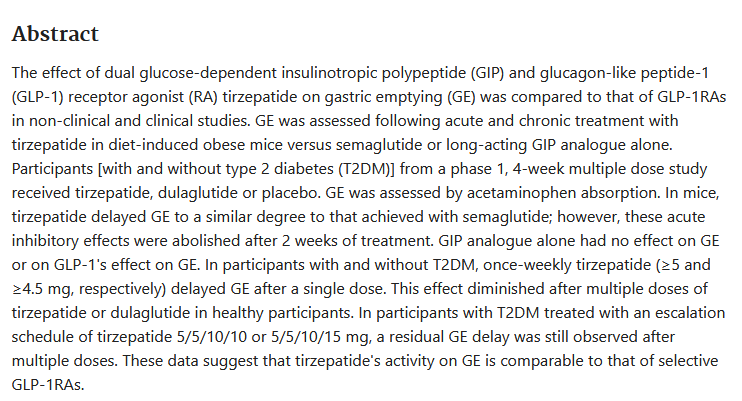
In other words, the delayed gastric emptying is a transitory effect, only lasting a few weeks. Meanwhile, the study went 40 weeks, and people lost weight the entire time.