Possibly?
Jonathan Swift Quote: “You cannot reason a person out of a position he did not reason himself into in the first place.”

Possibly?
Jonathan Swift Quote: “You cannot reason a person out of a position he did not reason himself into in the first place.”
Well, first, forgive a contradiction of “absolute garbage”–epidemiology is great in its proper sphere. It is simply that its sphere does not include the field of human nutrition. But epidemiology works quite well to establish the cause of a communicable disease or a chemical contamination. Let’s not forget that, please.
Bradford-Hill evolved his criteria for cases where RCT’s cannot be done, so that epidemiological data are all we have. It was he who made the convincing case that smoking tobacco causes lung cancer. I don’t want to go into all his criteria, but among other things, he required a strong effect size, one that was both clinically and statistically significant, a dose-dependent response, and a plausible mechanism of action, which are lacking in almost every epidemiological nutrition study.
In the case of cigarette smoking, smokers have (depending on the study) a 10-30 times greater risk of developing lung cancer than the non-smoking population, the risk of lung cancer rises steeply with the number of cigarettes smoked in a day (and I think the plausible mechanism is even more plausible, now that we know about the role of mitochondrial damage in promoting cancer). Taking all this into consideration, Bradford-Hill felt that we were justified in saying that smoking causes lung cancer, even on the basis of epidemiological data alone.
The “real” way to establish causality, of course, would be to have matched populations smoking different numbers of cigarettes–from zero, to a few, to a pack, up to several packs a day–and following them for thirty years to (a) make sure their smoking pattern didn’t change, and (b) determine the rate of lung cancer in each group. Enumerating the practical difficulties of performing such a study is left as an exercise for the reader. 
So in the case of smoking, where the absolute rate of lung cancer is, say, 3% in the non-smoking population, and 30-90% among smokers, it seems pretty clear that smoking is causal, especially since the data also meet all of Bradford-Hill’s other criteria. Likewise, Robert Lustig runs through similar logic where fructose is concerned, and claims a clinically significant increased risk, a dose-dependent response, and a couple of different mechanisms resulting in various diseases, so he feels justified in calling fructose a toxin. (And in the case of fructose, RCT’s also happen to be much easier to do, so there are additional data in support of the idea that fructose is toxic.) But again, the clinical effects in both cases are highly obvious, as compared to a 1.3 hazard ratio of eating red meat and developing colorectal cancer, to name one example.
In the case of statins, there is no doubt whatsoever that statins have a significant causal effect in lowering cholesterol. The problem arises from using cholesterol levels as a surrogate for cardiovascular disease, because the clinical effect of statins on rates of cardiac events is minuscule in absolute terms (and probably derives from their anti-inflammatory effects, not from the lowering of cholesterol). Hence the reason for promoting the relative risk reduction.
So the short answer is, yes, we need to know both relative and absolute risk when RCT’s are published, and yes, an epidemiological study isn’t even worth considering if the effect size is not at least 2.0 (and perhaps not even then).
“It is difficult to get a man to understand something, when his salary depends on his not understanding it.”—Upton Sinclair
My view is that statins do have a small benefit in preventing heart disease… but not by lowering cholesterol in any way. In fact, the cholesterol lowering makes things worse. But statins do reduce inflammation. What causes CVD? Inflammation. Of course it would be much better if you reduce inflammation naturally eg by not pouring carbs down yer neck… then you wouldn’t need any drugs.
My understanding is that statins have been shown to lower cholesterol of all size categories. To the extent they lower HDL in the process, they may well cause more harm than good over the long run.
Such a view would not be consistent with the studies I’ve read.
There is a small association between statin intake and reduced incidence of a secondary CVD event in adult males. That is not quite what “prevention” typically implies. But read on…
There is no support for statins being associated with a reduction in secondary CVD events in women.
There is no associative support that statins are effective at reducing primary CVD events in either gender.
Moreover, there is associative evidence that statins increase overall mortality across genders (i.e., after including other ways to die besides CVD events)… whether or not the patient has already had a primary (= first) CVD event.
I’ll dig up the relevant studies if interested.
The problem with any drug is that it will have multiple effects. To the extent that statins are beneficial, how can we know whether it’s due to lowering LDL or through some other effect?
Well, there are at least a few studies out there that answer this. In one, they looked at the amount LDL went down for a given statin (with the same dosage), and then stratified this. This occurs because not everyone gets the same LDL decrease, so you divide this into the LDL decrease you got. They found that higher LDL decreases did not correlate with better results.
In another test, they gave two different dosages of the same statin to people, and the higher dosage did lower LDL more, but again, no benefit to the outcomes.
So, it’s unlikely lowering LDL is what causes benefit from statins.
So, pleiotropic effects are probably what provides the benefits (if there are any).
Since our discussion here has morphed into one re: LDL and statins, I thought some of these might be of interest to anyone still following this exchange…
##############
Lack-InverseAssoc-LDL-Mortality-2015.pdf (881.6 KB)
“Conclusions: High LDL-C is inversely associated with mortality in most people over 60 years. This finding is inconsistent with the cholesterol hypothesis (ie, that cholesterol, particularly LDL-C, is inherently atherogenic).”
##############
MinnesotaCoronaryExperiment-FIRSTPAGE.pdf (332.8 KB)
"There was a 22% higher risk of death for each 30 mg/dL (0.78 mmol/L)
reduction in serum cholesterol…"
##############
StatinAdherence-CVD.pdf (413.4 KB)
“Our perspective of the literature is that non-adherence to statin treatment for primary prevention of CVD is justified because the meager benefits are more than offset by the extensive harms.”
##############
Statins-LowCarb-Aug22.pdf (552.9 KB)
"Summary
Extensive research has demonstrated the efficacy of the LCD [low carb diet] to improve the most robust CVD risk factors, such as hyperglycemia, hypertension, and atherogenic dyslipidemia. Our review of the literature indicates that statin therapy for both primary and secondary prevention of CVD is not warranted for individuals on an LCD with elevated LDL-C who have achieved a low triglyceride/HDL ratio."
##############
Atherosclerosis-Cholesterol-Causality.pdf (161.3 KB)
“…Nonetheless, degree of coronary calcification did not correlate with any lipid fraction in the blood… [P]rogression of atherosclerosis was associated with a decrease in cholesterol, not an increase… The role of LDL-cholesterol for atherosclerosis growth has been exaggerated, a finding with consequences for the prevention of cardiovascular disease… [A]lthough the presence of exposure-response is not sufficient proof in itself of causality, it is difficult to explain its absence.”
##############
All those papers are arguing that reducing LDL is not a good thing. No disagreement from me. My point was that there was a small benefit from statins of reducing inflammation.
Paper 3 did accept there were benefits of statins: calling them “meager” doesn’t reduce them to zero. Most people accept there are major side effects of statins, but again, this should not mean we simply ignore any potential benefit.
I personally would never take a statin and I am no statin apologist. But we do have to think a bit about the various RCTs on statins that do show a marginal benefit, and ask why.
This appears to be so. But as you point out, there are better ways.
The problem with statins is really the side effects, such as myalgia, cognitive impairment, impotence (also known by the prissier new term “erectile dysfunction”), Type II diabetes, cancer, and so forth.
Interestingly, Professor Sir Rory Collins at Oxford claims that almost no one experiences side-effects from taking statins, but the company he formed to market his gene test for vulnerability to statin side effects claims that at least 25% of people taking statins experience side effects. Fascinating!
Perhaps another reason to ask why there may well be some benefit from statins is that Pharma can’t get approval for a substance that lacks any benefit whatsoever - even if side effects and long term risks are significant.
In fairness, even crack cocaine provides certain benefits - including weight loss.
Well, the reasons for this are complex. One is the constant use of relative risks for any “benefits”, which blow up the benefits, since the denominator isn’t provided. Another is using absolute risks for any side effects, which minimizes the amount of side effects. Yet another is splitting side effects into many small side effects, so they don’t “add up” to anything substantial.
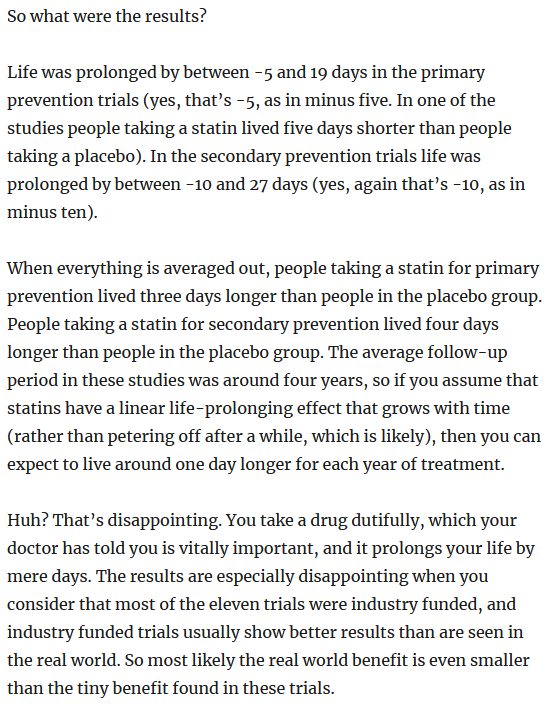
But often I wonder this myself. Here’s an overview of a study from 2015:
I guess no one, particularly doctors pushing these drugs, reads these studies.
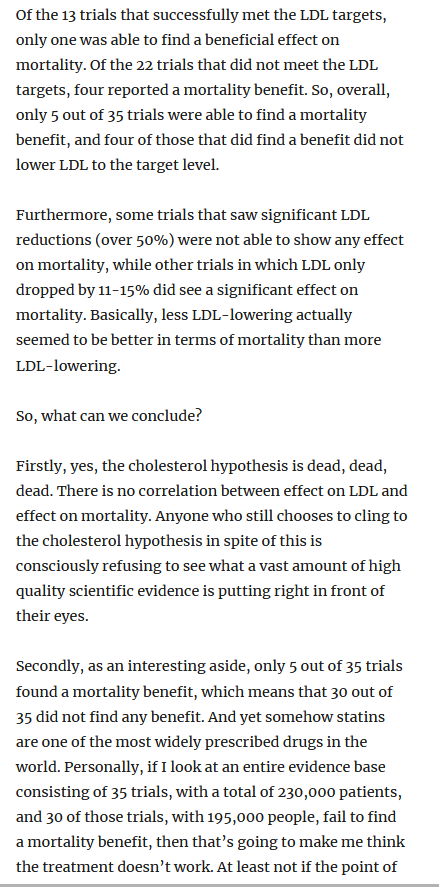
Edit. I never heard of that person before, but he has some good articles. Here’s another:
I brought this up to my husband’s doctor who wanted to put him on a statin. His counter was that it’s not quantity as much as quality. Any thots? How is “quality” calculated?
I have no clue what that doctor is trying to say. It’s not the dosage of statins but how potent they are? It’s not about how many doctors are in a room, but how good they are?
Sorry, I’m lost with what this doc was getting at. 
Oh, lol. Quality of life, sorry! Like we’ll finish the race neck in neck, but he’ll have had a higher quality of life than I, due to the statins.
Ah, thanks for the clarification! … that makes (a bit more) sense 
So it seems his doc is saying that a statin will make him enjoy life and feel better than he would without them - a quality of life thing.
Apparently his doc hasn’t read the statin label - contraindications and highly common side effects. Nor read any studies beyond what he recalls during Powerpoint presentations at those drug company-sponsored free dinners.
Related: A dead giveaway for me is how many of those drug company dinners that doctors are lured to feature pics of thick juicy glistening steaks as the marketing draw.
Yeah, cholesterol control, sure.