
@Knnn Let us know how you respond.
Parkinson’s and Exogenous Ketone Esters
daddyoh
(Eric - The patient needs to be patient!)
#14
Maybe there is some logic here that will work: How can keto be worse than parkinsons. If after 2 months he does not get relief from keto them go back. Seems very odd that a diet would be worse than parkinson’s in someone’s mind.
BuckRimfire
(BuckRimfire)
#15
Yes, it would be one thing if you had mild acne and thought a keto diet might help. Then, if someone really thought the diet was risky, they might have a case, but OH WAIT, DON’T TRY TO SAVE YOUR MOTOR SKILLS, YOU MIGHT GET HIGH CHOLESTEROL!!!
#massive eyeroll
Knnn
(Ian)
#16
My friend and I tried a Ketone ester which contains 25 g of BHB ester (I believe) and these are our blood ketone levels (measured with a Keto Mojo):
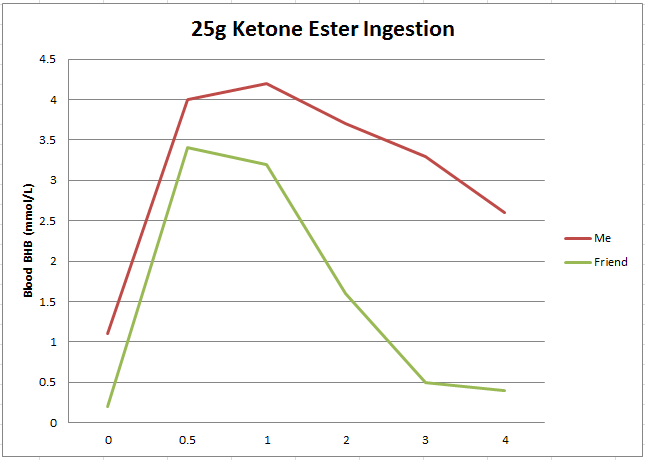
As you can see from the graph, I was already in a state of ketosis and have been for approximately 12 months. My friend who is suffering from Parkinson’s, has never been in ketosis (except presumably when he was a baby).
He consumed the KE after his conventional medication had worn off, to determine if he could feel any affect. Within approximately 15-20 minutes he noted more mental clarity than he would expect, which lasted for approximately 1 hour. Between 30 and 60 minutes he also noticed brief periods of tingling (almost but not quite pins and needles) in his extremities, which he said was similar to the effect his conventional treatment had.
My friend does not have the conventional Parkinson shakes that is seen in the video by William Curtis, as shown above. He experiences cloudy thinking, lose of feeling, poor temperature regulation (extremities get very cold), stiffness and any movement becomes an effort that has to be consciously thought about. While the elevated blood BHB appeared to provide some relief, it was not as effective as his medication.
I had assumed that I would consume my BHB quicker as I am already fat adapted and my body is ready and very able to use blood ketones. However, I was surprised to see that while we had a somewhat comparable increase in blood ketones (his was 0.2 to 3.4, a net gain of 3.2 mmol/L and mine was 1.1 to 4.0, a net gain of 3.9 mmol/L), his ketone levels fell earlier and far quicker than mine, almost as though there was a higher demand?
Considering that there appeared to be some physiological benefits between 0-1hour after consuming the KE, when his blood ketone levels were the highest, I am left wondering if there is room for improvement, i.e. if continued consumption of more KE over time to keep the BHB above 4 or 5 for a prolonged period of time? For example, an initial dose of 25 g and then 3 further half does of 12.5 g every hour.
Also it may be worth trying to elevated BHB levels in conjunction with his medication, however, this is something that should probably be tried with medical supervision.
Does anyone know if there is a maximum recommended dosage?
Any thoughts would be most appreciated?
PS, it was interesting to note that after 4 hours, when my BHB was still at 2.6, my blood glucose was down from an initial value of 5.1 mmol/L to 3.4 mmol/L, which is quite the Dr.Boz ratio.
goohsmom
(PSackmann)
#17
Thank you for posting your results @Knnn. My husband is suffering from short-term memory loss and a lack of clarity lately, but he is resistant to the idea of a keto diet as he loves sugar. I had contemplated picking up some MCT oil or KE for him to try, I see from your results that he’s likely to have to take the KE continuously to get the same effect as being in nutritional ketosis.
carolT
#19
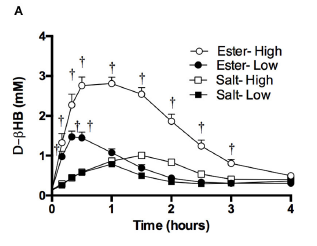
I found a study (pdf available) where they are measuring such things in the context of humans. (There are a boatload in rodents but the numbers aren’t always indicative of human reactions.) The typical peak and dip lasts about 3 hours feeding of BHB as ketone ester (141 mg/kg and 282 mg/kg of R-3-hydroxybutyl-R-1,3-hydroxybutyrate) dosed according to bodyweight. The higher dose produced a steeper curve, but duration was about the same.
Then they looked at how often they needed to feed the ester to achieve specific levels:
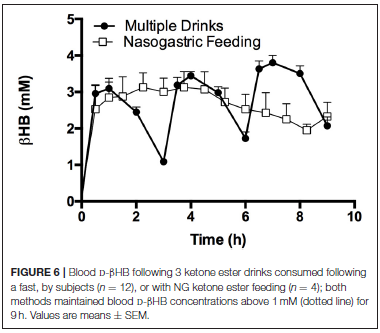
So, there is a bit of buildup with successive feedings, but there’s still peaks and dips compared to a constant influx with a feeding tube. As mentioned above, the transport across the BBB differs by individual, so it’s important to figure out what plasma level needs to be achieved for the desired results. I have to think the supplements will get expensive and at some point maybe they’ll be more receptive to a dietary intervention.
The other thing you might want try is extending the BHB window using MCT oil, if their gut can handle it. I’ll see if I can find a human study on that. It might give you a less drastic rollercoaster.
Yes, one of the side-effects of exogenous ketones is a corresponding reduction in glucose. If you are using an ester, there will be acetoacetate present in addition to the BHB you can test with the meter. Both of these are used by the brain and compensate for glucose as an energy source. The high level of ketones alter the pancreatic hormones to lower glucose.
carolT
#20
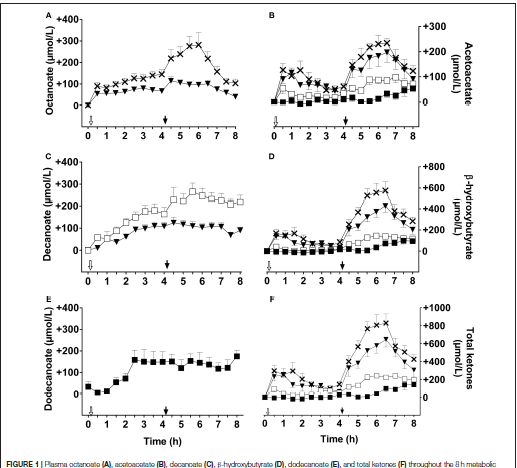
Oh good, here’s the effect of MCT oil over an 8 hour period. The study is broken down into the 3 specific fatty acids, C8, C10, C12 by their rate of absorption and BHB increase. Their conclusion is that C8 has the most effect.
Combining MCT and esters might be a good strategy for your friend? The bump in ketones from MCT oil isn’t nearly as high and large doses generally cause the gut to rebel.
AUCs for plasma total ketones were not significantly different
between C8 and C8C10. Compared to C10 given alone, both
C8 and C8C10 increased the AUCs for plasma AcAc by 2 fold,
plasma b-HB by 5 fold and total ketones by 2.5 fold
P.S.
The C8 oil Brain Octane is more expensive than regular MCT oil, but may/may not give you a bigger boost at a tolerable ingestion level.
PaulL
(You've tried everything else; why not try bacon?)
#21
That certainly sounds reasonable.
The one caveat I would put forward is that there is no research, so far as I know, to demonstrate what happens when exogenous ketones are consumed in a state of high insulin. Harm doesn’t seem likely, but I don’t believe we know for sure. @carolT? Anything you might add? I’m not spotting anything on PubMed.
Though your friend’s experience demonstrates that they do get into the brain, at least.
daddyoh
(Eric - The patient needs to be patient!)
#22
Paul this is a great point. We just don’t know. I’m learning so much from this thread and others for topics that don’t directly apply to me. Thanks, @PaulL @carolT @atomicspacebunny and others for your science perspective.
carolT
#23
Hmmm… exogenous ketones bypass the regulatory effect of insulin on their production, not that it’s an issue since he’s not producing any of his own. Ketones still have an inhibitory effect on lipolysis through the HCA2 receptor in adipose tissue, but also play an anti-inflammatory role in the body.
As to any dangers of combining ketones and insulin… I can’t think of any off hand. It would be glucose or acidosis to worry about more?
daddyoh
(Eric - The patient needs to be patient!)
#24
Two people that might have an answer are https://twitter.com/DominicDAgosti2 Dom D’Agostino and Geoffrey Woo https://twitter.com/hvmn
Both sell exogenous ketones but I think both would give you links to research. I probably trust Dom D’Agostino more since he started out just as a researcher. Is in follow the money.
carolT
#25
Found some data on insulin reducing ketones directly compared to just lowering production. So the faster clearance could be partially due to higher insulin.
The sodium acetoacetate infusion rate required during the clamp was 55 % higher during hyperinsulinaemia than in controls. This was due to increased total ketone body clearance (8.4 vs 6.7 ml. kg -1.min -1) and to enhanced suppression of ketone body production.
…
Since the plasma insulin concentrations were within those observed in patients treated for diabetic ketoacidosis, the data suggest that the antiketotic effect of insulin therapy results in part from an increase in peripheral ketone body disposal. http://www.springerlink.com/index/V548062016529563.pdf
P.S.
Frankly, I’d be way more worried about giving high dose exogenous ketones to someone with LOW insulin.
KetoCancerMom
(Cancer Fighting Ketovore :))
#26
Why? And how high is “high dose”?
I’m trying to keep my ketones up with MCT oil, and I’m trying to find the right balance of how much MCT oil at a time and how frequently to take it. I’ve wondered if ketone salts or esters would be better.
carolT
#27
I’ll define high dose as using more than what’s instructed on the label (for esters) that gives you an increase beyond physiological normal ranges for fasting. So, if bumping the dose puts you at like 5 or 6 mmol, then that’s fine. By low insulin, I mean like not producing enough, or borderline T1. One of those in-between diagnoses you don’t hear much about.
I think the decrease in glucose seen with esters is waranted for cancer therapy as well, but it’s only part of the treatment.
As you can see from the chart I posted above, salts don’t give you much different levels than MCT.
KetoCancerMom
(Cancer Fighting Ketovore :))
#28
I’m just trying to find what will work best. Sometimes it feels so hit-and-miss. I may try to just regularly take ½ tablespoon of MCT oil several times a day.
I’m also hoping that glucose levels will go down more once the kids go back to school.
carolT
#29
MCT is certainly cheaper. How much can you tolerate without the dreaded “gastric distress”? I can take up to 2 tbsp and be ok as long as I don’t take any more for about 6 hours.
KetoCancerMom
(Cancer Fighting Ketovore :))
#30
I’m not sure. I haven’t really tried. But it might be 2-3tbsp. I may try it one day when I’ll be home all day 
PaulL
(You've tried everything else; why not try bacon?)
#31
I can’t either, as it happens, but that doesn’t mean there aren’t any. If I were a researcher, my hypothesis would be that exogenous ketones cause no harm, but I’d want to do a large, well-funded study, just to make sure! 
carolT
#32
Are you asking about taking exogenous ketones with exogenous insulin? I don’t recall seeing any studies like that either. Most of the studies using ketone esters are for people who can’t or won’t do a keto diet, so have normal (for SAD) insulin. Or rats.
Knnn
(Ian)
#33
I cant express how much I appreciate all these very interesting and informative discussions. Thanks.
My friend tends to cook everything from whole foods and eats very little processed foods. His blood work indicates that he is not pre-diabetic or diabetic, so I anticipate his insulin levels will be relatively normal, whatever that is defined as these days .
As Carol points out, I am hoping that he feels enough improvement with exogenous ketones to encourage him to consider trying a ketogenic diet or even therapeutic ketosis to help mitigate symptoms or disease progression.
Considering how much my blood glucose level was reduced with the consumption of a single dose of exogenous ketones (down to 3.4 mmol/L), is there a potential concern that inducing a higher level of exogenous ketones over a longer period of time (such as by repeated dosing through the day), would result in dangerously low blood glucose post treatment, i.e. after the ketone wore off?
I am speculating that for me it would probably not be an issue because my body is already producing endogenous ketones to compensate from reduced blood sugar, but for my friend who is not adapted to fat burning, it might be an issue?