@atomicspacebunny Thanks for your thoughtful reply. (You do ask a lot of questions  , but I’ll take on two…)
, but I’ll take on two…)
This is perhaps the central question, right? It comes down to context. If you’ve got both: (saturated) fat and carbs competing for your metabolism’s attention at the same time, the outcome will not likely be pretty. One might get a vastly different outcome if there were little if any carbs in the mix (i.e., a ketogenic foodstyle, as is well known throughout this forum).
Yeah, it would seem there’s some distinction between the LMHRs and the non-LMHRs groups … and genetics may well be a key component.
After all, since both groups appear to be eating largely the same keto-oriented diet, and one group sees a slight lowering or perhaps stable serum LDL, while the other sees this remarkable spike in LDL-P and/or LDL-C (concordant vs discordant possibilities), it’s probably not the diet - it’s the human genetic predisposition (?)
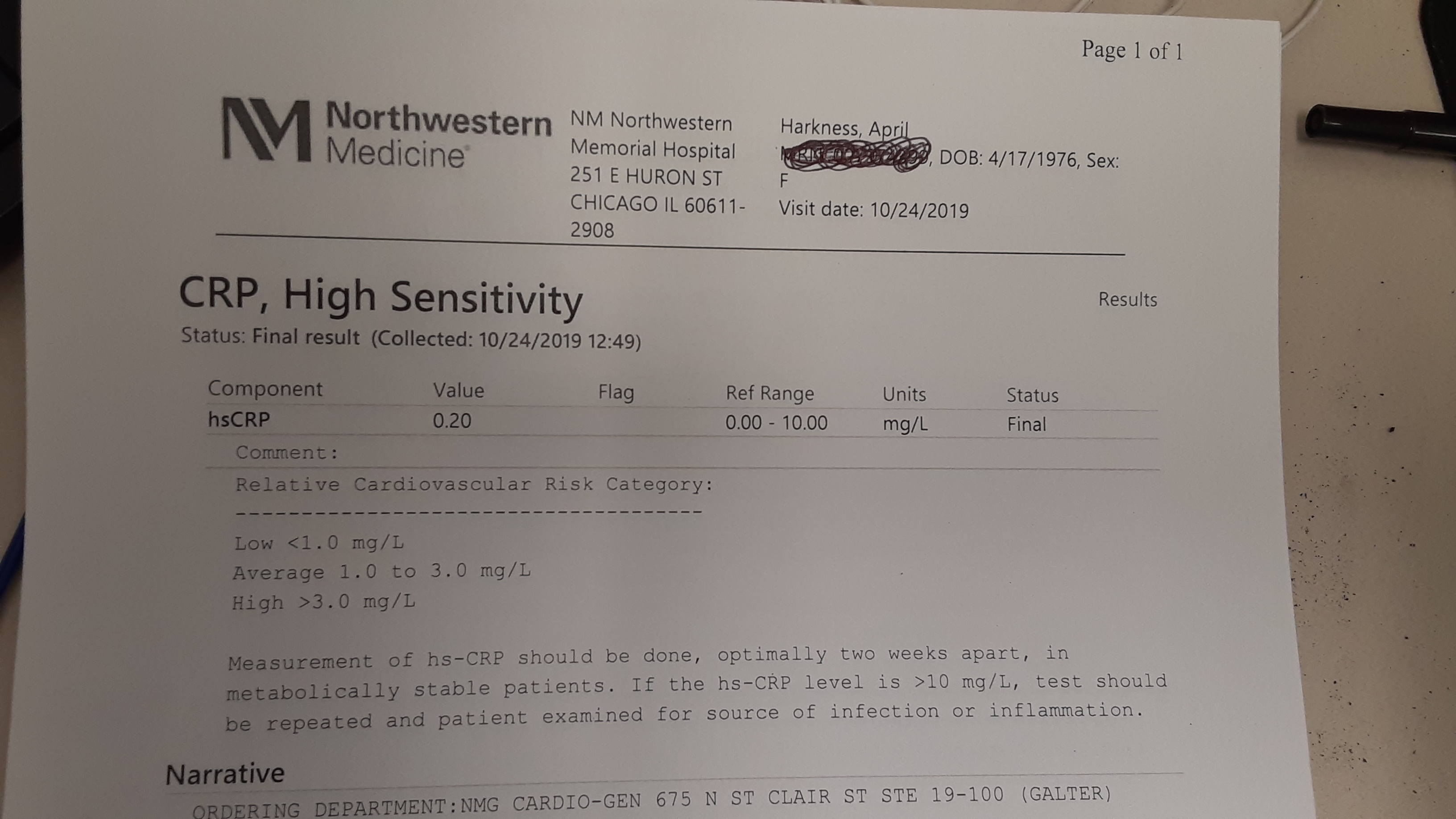
I’m not sure why you mention inflammation though. Personally, as an LMHR I see no indications of inflammation whatsoever - especially as compared to the achy/stiff muscle/joint discomfort I suffered from previously while dutifully eating low fat and “healthy” complex carbs.
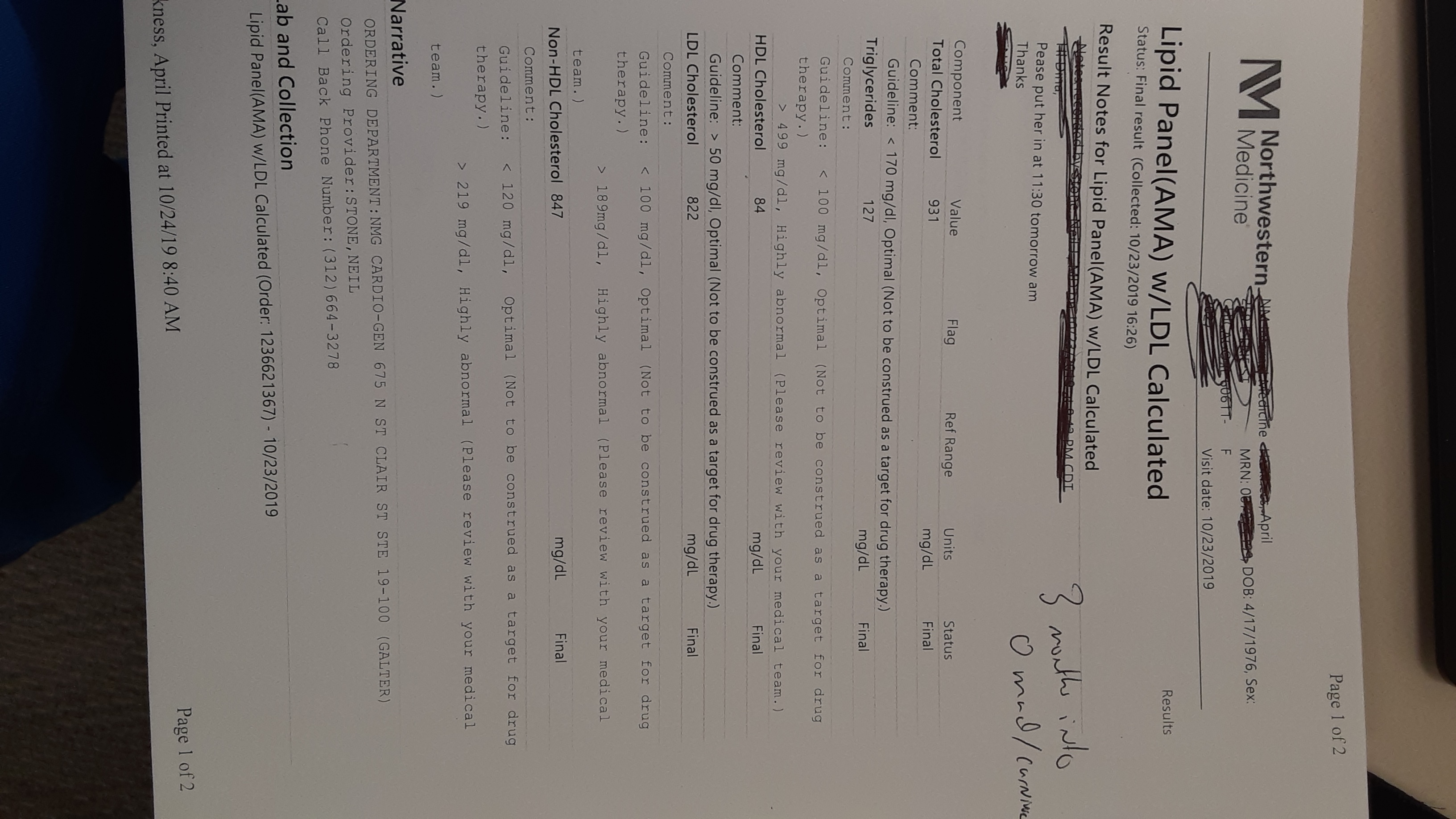
But, being one of those LMHRs with concordance (both my LDL-C and LDL-P have “spiked nicely”), I’m left scratching my head. Yet, all the while I feel better than I have in decades. And all my other lipid markers, blood pressure, serum glucose/ketones, weight, girth, musculature, etc., all improved.
As for saturated fats (vs PUFA and MUFA), being a data geek, my detailed daily logs indicate that my intake has represented roughly 25-35g/day on average … i.e., roughly 25% of my total daily fat intake. So, as long as I’m continuing to eat those healthy animal-derived fats, there’s not much I can do to lower the % of saturated fat.
Then again, these same experts also embrace the conclusion that concerns about natural, whole-sourced saturated fats were never science-based in the first place - when evaluated in the absence of carbs getting in the way … which I believe was your original point?
Onward! 


 Thank you
Thank you