
Buy him a … errr … The book
One way to approach this conversation, is to buy your doctor a copy of “Art and Science” which was designed for a technical audience.
Be the change you want to see
Another is to make sure they test your HbA1c (average glucose control over 3 months) then go keto and go back 3 months later for another test. What is likely to happen is they should see a dramatic drop in your glucose down to normal levels - and that can be an opportunity to have a conversation.
I suspect the evidence of your fat loss and lean gain, and your blood diagnostics may convince your GP that at the very least it helps lose weight and doesn’t appear to derange lipids outrageously as the conventional thinking on High fats diets might expect.
NOTE: I would not recommend going on a ketogenic diet prior to telling your doctor if you are on ANY medication to treat diabetes because diabetic medication may over correct and take your glucose TOO low.
But lets say your doctor doesn’t have time to read a book, and you are going to have the conversation BEFORE you go keto …
How do you explain to them a ketogenic diet.
I think if you are a type 2 diabetic it is worth explaining the homeostasis of glucose control. Your doctor likely knows this, they learned it in medical school, they may have just forgotten it.
Insulin clears glucose - that’s the upper range homeostatic regulator.
The liver makes glucose - that’s the lower range homeostatic regulator.
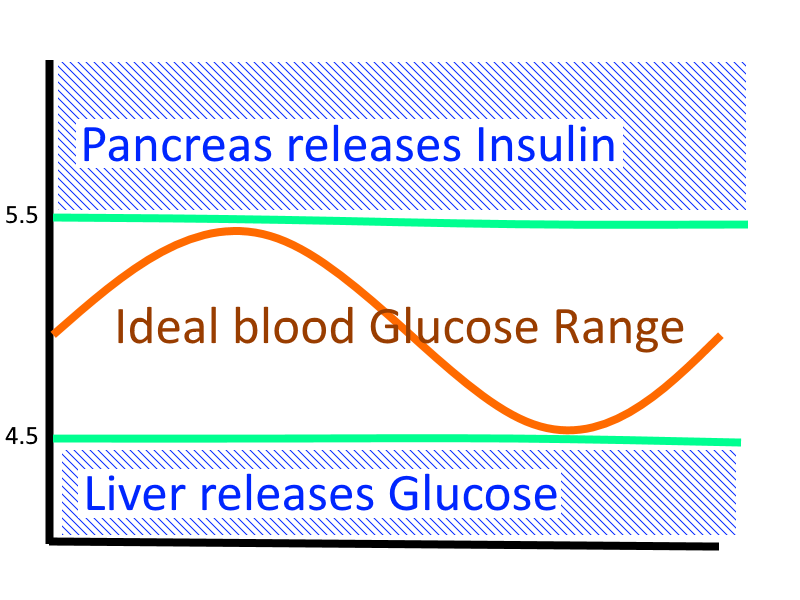
These two organs work together to keep your blood glucose in the ideal physiological range which is roughly between 4.5 and 5.5 mmol/l.
When you eat food that your body digests into glucose … essentially foods containing Sugar or Starch then in a healthy person their pancreas kicks into gear and releases Insulin to lower glucose. Insulin does a lot more but for the purpose of your glycostasis it’s primary effect is to clear glucose from circulation. When you go to sleep at night and you aren’t eating any foods that contain Sugar or Starch … then if your blood glucose goes low your liver releases some from it’s short term storage (glycogen) and it makes some more.
That ideal blood glucose range is key to keeping your brain functioning. When that goes too low your brain runs out of energy and you can slip into a coma. The fact that we don’t slip into a coma every night when we sleep indicates that our livers are doing their job.
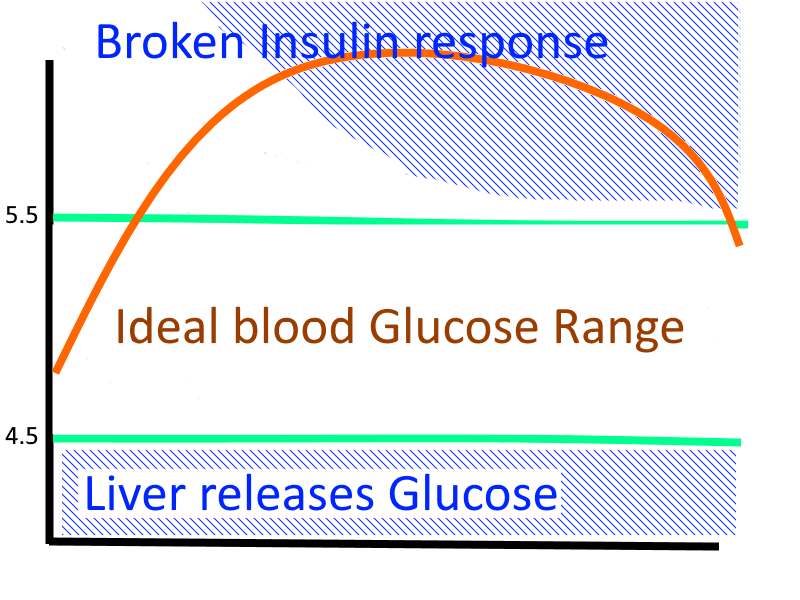
If your ability to make/use insulin is broken, and you eat foods containing sugar or starch then your blood glucose goes too high and stays up there for too long and that causes it’s own bad effects such as doing damage to the linings of your blood vessels, and sticking to proteins in your body making them misbehave.
The primary purpose of a ketogenic diet therefore is to keep your glucose at the low end of the range by not eating any sugar or starch and let your liver make glucose on demand and keep you in the safe zone.
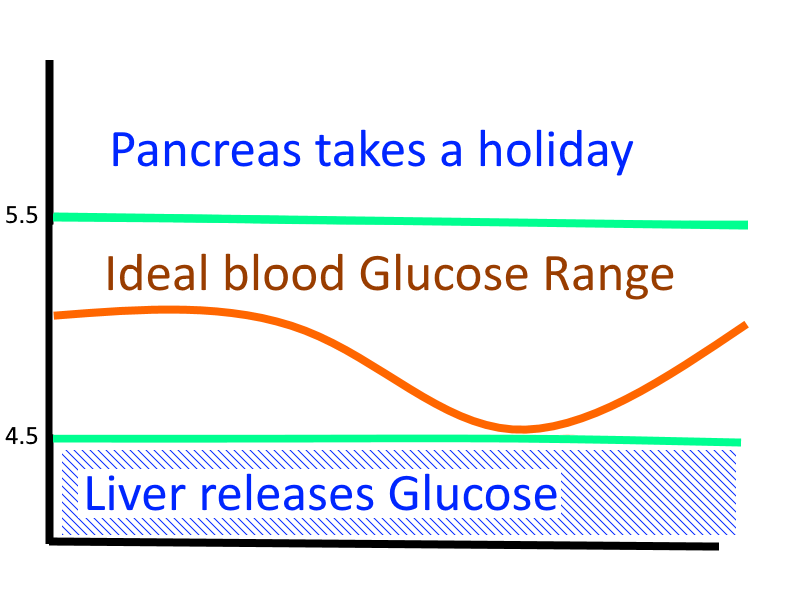
A patient who is making glucose on demand in their liver will be keeping their glucose in that safe physiological range as long as they don’t eat Sugar or Starch (and eat sufficient protein for the liver to turn into Glucose).
So about Diabetic medication
There are roughly 4 kinds of Diabetic medication;
- Medications that cause you to absorb less glucose from food
- Alpha-glucosidase inhibitors (acarbose)
- Medications that cause you to dump glucose already in your blood
- SGLT-2 inhibitors lower the renal threshold pushing glucose into urine
- Glifozin (dapagliflozin, canagliflozin and empagliflozin)
- Medications that cause you to have more insulin
- Injecting Insulin is obviously one
- Direct Insulin Secretagogues
- Sulfonylureas (glipizide, glyburide, glimepiride, and others)
- Meglitinides (repaglinide, nateglinide)
- Incrtetin mimetics
- Exenatide (Byetta)
- DPP-4 inhibitors like sitagliptin (Januvia)
- Medications that cause you to be more sensitive to the insulin you have
- Biguanides like Metformin (AKA Glucophage, Diabex)
- Glitazones like Avandia or Actos
Any of these that lower glucose already in the blood may overshoot in the context of a patient who suddenly has normal glucose levels by not eating any. Also any medication that increases insulin in the context of someone who already has blood glucose at the bottom end of the physiological range, is likely to overshoot their glucose into hypoglycemic ranges. So Category 2 and Category 3 diabetic medications almost certainly will have to be reduced as the patients glucose levels become normal.
Medications that reduce glucose transport across the gut (Category 1) are likely irrelevant in this context as the patient isn’t going to be absorbing much glucose.
Finally Metformin reduces the amount of glucose produced by the liver by around 30%, but this is apparently not sufficient to prevent it producing glucose on demand in response to low glucose events. What Metformin can be useful for is increasing the clearance rate of insulin, lowering chronic exposure, and reducing underlying insulin resistance. Which may allow type 2 diabetics to become more insulin sensitive over time, independent from their glycostatic control.
The standard of care
The standard approach to failing glycostasis is to medicate the patient with one of the above medications until their glucose control is in a range that is safely above the hypoglycemic range - this normally means to 7% HbA1c because these medications are an imprecise tool and we are rightly too scared of hypoglycemia to medicate them into the safe zone between 5% and 5.5% in case that medication overshoots people into comas.
Blood glucose over 6.1 mmol/l causes beta cells to be killed by glycotoxicity faster than they can replicate.
So the standard of care is literally to progress the disease as slowly as we can until the type 2 patient is insulin dependent. And every 1% rise in HbA1c is a 21% rise in complications from diabetes, 37% increase in microvascular disease, and 14% rise in myocardial infarcts.
Treating diabetes with Diet
By treating diabetes with diet, patients are relying on homeostatic mechanism that have finer control over the mechanisms than our pharmaceutical interventions. With diet patients can regress the disease, because they are able to achieve stable glucose by not eating any and making it on demand.
That is the case for not eating carbs if you are Diabetic.
The case for a high fat diet is more complex and a story for another day, but at the very least the mechanism of a low carbohydrate diet to control glucose lowers the risk of cardio vascular disease more than the worst projections for dietary saturated purportedly raise those risks (and there is significant controversy around those projections).

 thanks
thanks