
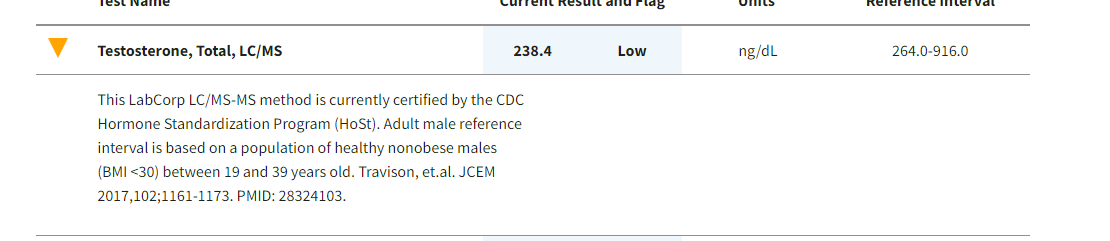
@fitbod Not to pick on your “low” Tot Testosterone, at least as it’s reported, but these “Reference Ranges” always crack me up.
As you likely know, they are typically structured to represent +/- 3 standard deviations (capturing 95%) or +/- 2 s.d. (to capture 85%) of the population at large.
Implications? Well, ask yourself…
Are 85% to 95% of the general population healthy?
Public health stats strongly suggest that, no, they are not. Upwards of 70% are suffering from some variation of obesity, diabetes or metabolic syndrome.
So every time I see some lab result of mine that’s outside the “Reference Range” I ask myself:
“Am I glad to be outside the zone where 85%-95% of my neighbors fall on this metric? Or would I prefer to have the same blood levels that these folks have?” 


 and it turns out I could have prevented this by keeping that line lower? Let’s say a very healthy Mediterranean style diet. We have all seen the blue zones longivity argument I am sure. My partners granddad lived to 95 perfectly healthy till the last couple months when he stopped eating when he felt his time had come. He ate meats, grains, legumes and fats every meal. Maybe he was blessed with fantastic genetics. Once again highly anecdotal and a worthless N=1 example but I think that now wants to make me want to be open minded and look into both sides more and very carefully. If someone is diabetic, I don’t have a pinch of doubt keto is the way to go. Some one that is NOT diabetic or epliptic? IDK anymore. I have shared this, perhaps useless, anecdote earlier in this thread- My partner is vegan, but eats fish couple times a month (vegan-pescatarian diet). High carb diet obviously. His TG, LDL, HDL are fantastic. His last A1C was 4.5. He is even in ketosis after over night fasting and skipping breakfast, I made him check once out of curiosity. . My numbers are all good, except the typical high LDL that us Keto folks tend to have. I did NMR which came back excellent. So not worried about LDL anymore. But my darn A1C crept up to 5.7, prediabetes. So why should I blindly assume (for myself only) that Keto is better ( despite becoming pre diabetic ) than, let’s say, healthy pescatarian, unless I have health conditions and allergies, which I currently don’t have any? I am obviously biased towards Keto because of it’s otherwise proven benefits, which I have experienced . So I hope keto is indeed the best for longivity as well! Since there is no research, I welcome any reasonable anecdotal experience. Tagging
and it turns out I could have prevented this by keeping that line lower? Let’s say a very healthy Mediterranean style diet. We have all seen the blue zones longivity argument I am sure. My partners granddad lived to 95 perfectly healthy till the last couple months when he stopped eating when he felt his time had come. He ate meats, grains, legumes and fats every meal. Maybe he was blessed with fantastic genetics. Once again highly anecdotal and a worthless N=1 example but I think that now wants to make me want to be open minded and look into both sides more and very carefully. If someone is diabetic, I don’t have a pinch of doubt keto is the way to go. Some one that is NOT diabetic or epliptic? IDK anymore. I have shared this, perhaps useless, anecdote earlier in this thread- My partner is vegan, but eats fish couple times a month (vegan-pescatarian diet). High carb diet obviously. His TG, LDL, HDL are fantastic. His last A1C was 4.5. He is even in ketosis after over night fasting and skipping breakfast, I made him check once out of curiosity. . My numbers are all good, except the typical high LDL that us Keto folks tend to have. I did NMR which came back excellent. So not worried about LDL anymore. But my darn A1C crept up to 5.7, prediabetes. So why should I blindly assume (for myself only) that Keto is better ( despite becoming pre diabetic ) than, let’s say, healthy pescatarian, unless I have health conditions and allergies, which I currently don’t have any? I am obviously biased towards Keto because of it’s otherwise proven benefits, which I have experienced . So I hope keto is indeed the best for longivity as well! Since there is no research, I welcome any reasonable anecdotal experience. Tagging