Well, I can already see one thing I read wrong: N=16; the intervention arms each started with 13 people, and then
Overall, one patient dropped out during the KD intervention, four patients during MD, and five patients during the washout period. In total, sixteen patients completed this study and were included in the final analysis
So there is still going to be a low signal/noise ratio.
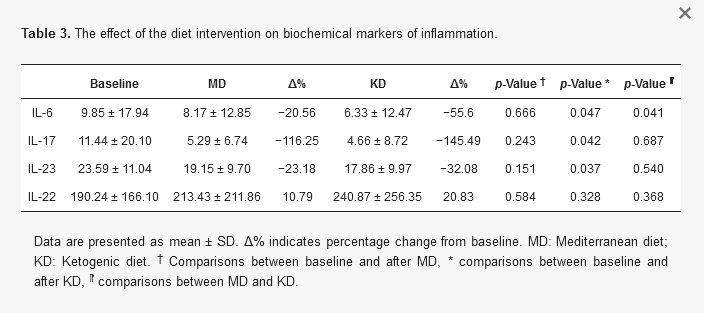
The weight reductions from the two diets were both statistically and clinically significant. The Mediterranean diet weight loss was around 7 kg, the keto loss around 10 kg. Both are great enough to be noticeable. Most of the biochemical markers measured did not change significantly. The keto diet produced a drop in triglycerides, but it was not statistically significant, to my way of thinking, at least. The authors seem to think that a p <= 0.05 is significant; whereas the statisticians John Ioannidis and David Colquhoun argue strenuously against this as a gross misunderstanding of what the p-value tells us. CERN, by contrast, looks for 6-σ deviations from the mean, which is p < 0.0001 (if I got that right).
The researchers notice a reduction in the participants’ PASI and DAPSA scores, which measure the severity of psoriasis and of psoriatic arthritis, respectively. However, their p-value is 0.04, which . . . .
The remark in my earlier post about not continuing the study long enough to see results is both true and misleading. Obviously, the study lasted long enough for the reasearchers to see some benefit from the diets (more from keto, yay!), but my own experience with seasonal eczema and rheumatoid arthritis suggests that a year would not have been too long to study the participants.
So all in all, I’d call this an encouraging pilot study, and reiterate the usual comment that “further research is needed.”