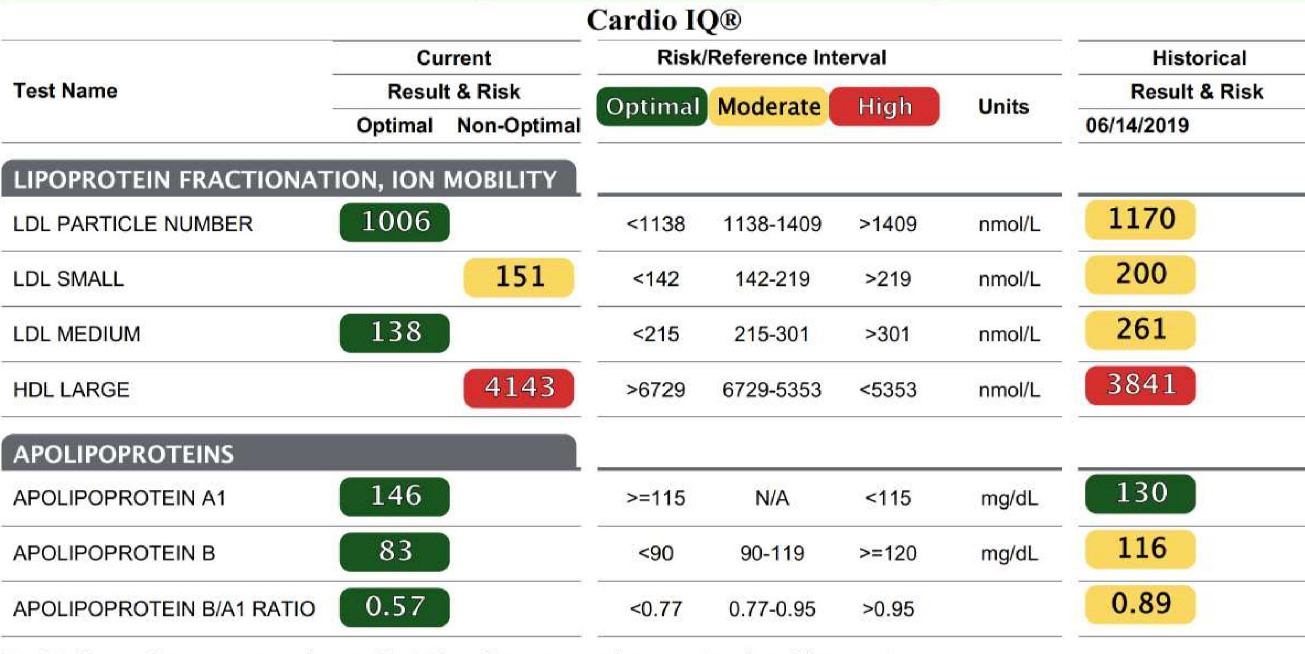
Lab test results for ApoB in my care system are reported in mg/dL, but in publications they’re often in molarity (e.g. nanomoles per liter). Anyone know the conversion factor?
I could just look up the molecular weight of an ApoB protein and do it directly from that value, but I’m wondering if there is something about the measurement/reporting method that would confound that.
In fact, I tried doing that from my ApoB test result (which was near the middle of the “normal” range), and got 23 microM (23,000 nanoM), which is ridiculous! And 2300 nM would be extremely high, while 230 nM would be impossibly low, so I doubt I’ve made an order-of-magnitude error.