The Collaborative Science Conference was a success.
I am seeing a changing of the guard. My first forays into keto conferences were all about weight loss but shortly was followed by the T2D reversal. The nature of The Cholesterol Code and Citizen Scientist might have some impact, but I am seeing more and more a focus on cardiovascular disease and diabetes as the driver to that. SO, this conference really was focused on lipids, CVD and mental health.
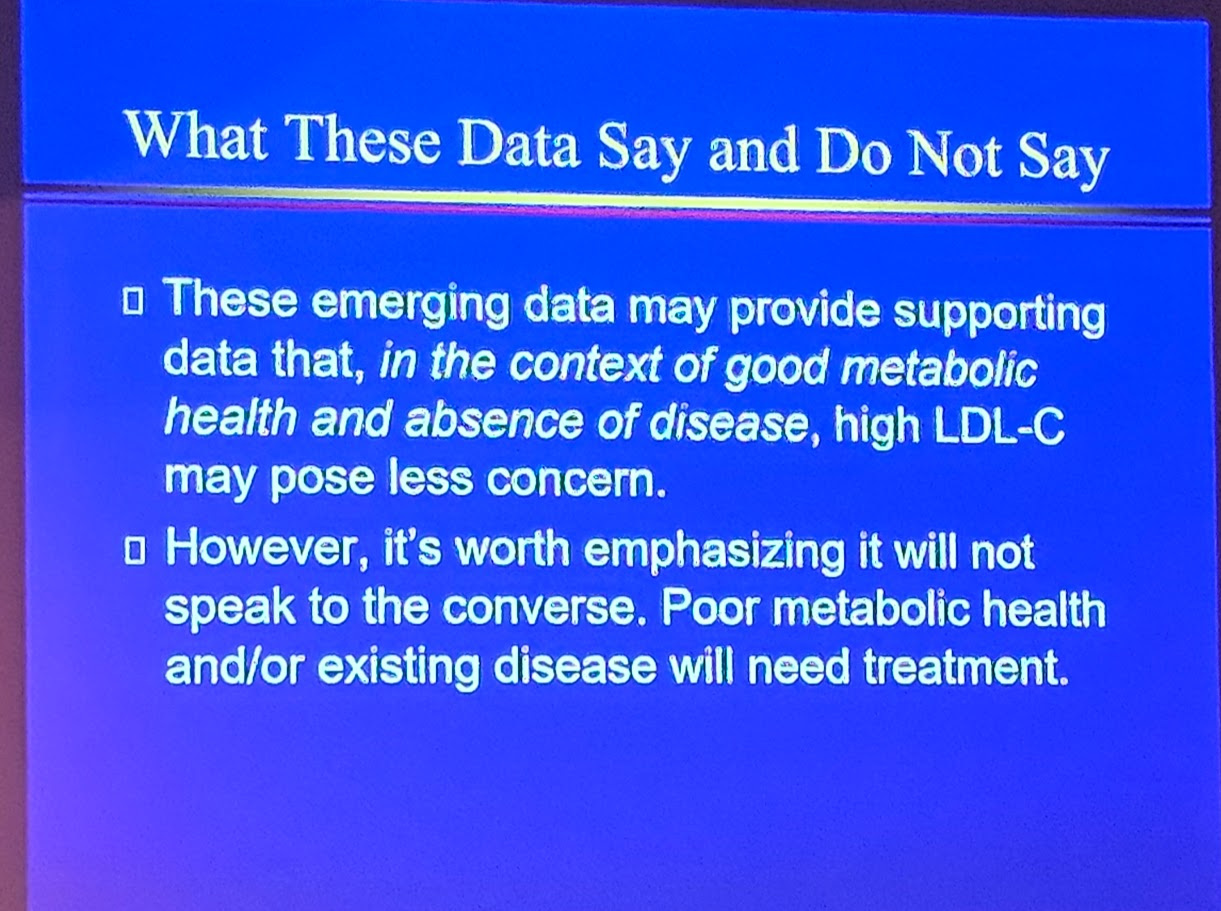
Matthew Buddoff presented Citizen Science LMHR study and there was no correlation between plaque burden and LDL-C, furthermore, subjects on a ketogenic diet did not have greater plaque burden as compared to Miami cohort study. However, the cognitive dissonance resonated and reigned as Buddoff was still willing to prescribe statins.
![image|690x388]
(upload://qZQqgZoVZra0dp59L2yWfUTlAD0.jpeg)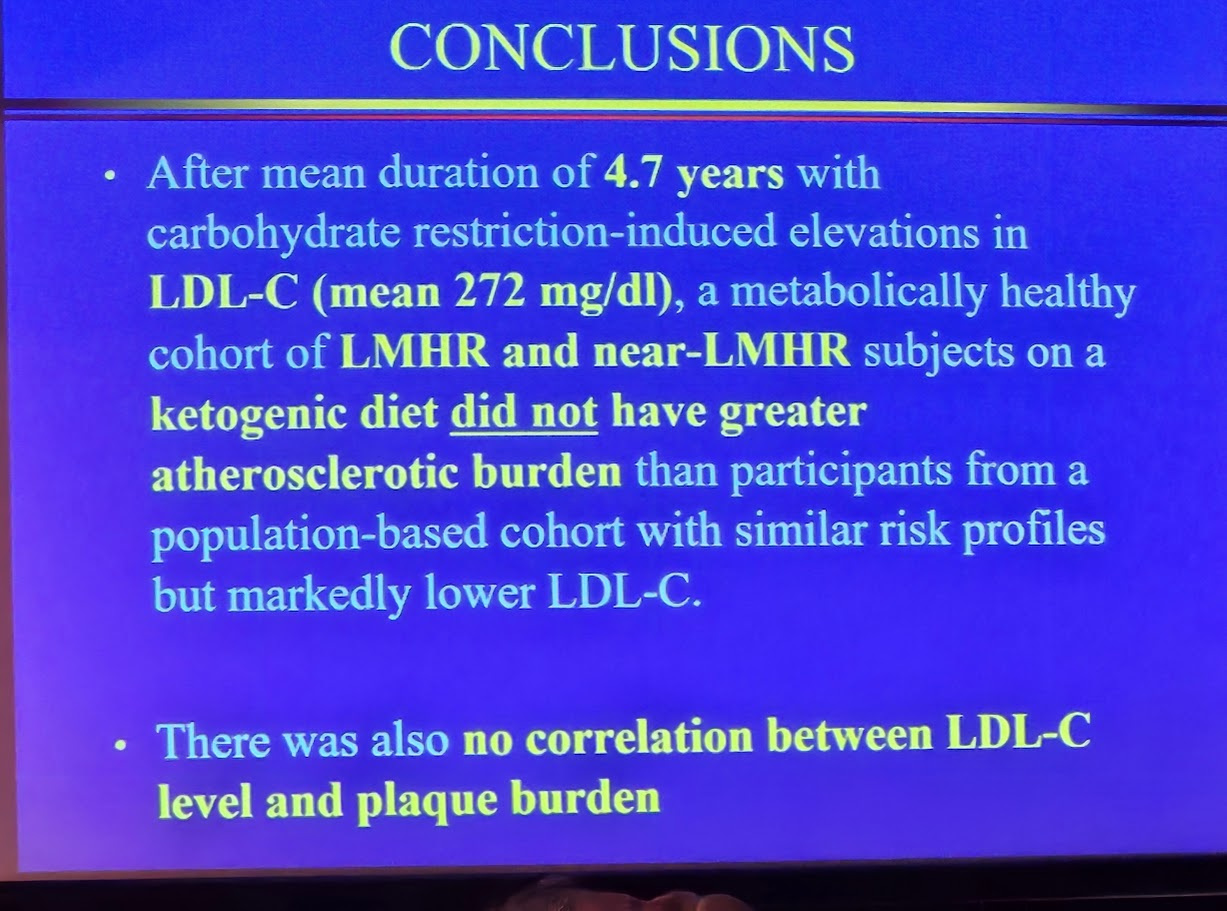
Cromwell presentation was great. He has a variety of ways of measuring CVD risk ruling out LDL, but recommended statin therapy still. Nadir Ali challenged him, rather convincingly on this during a panel discussion that lasted 90 minutes and was moderated by Feldman. Bret Scher maintained a more nuanced position but did not recommend statins, in most cases.
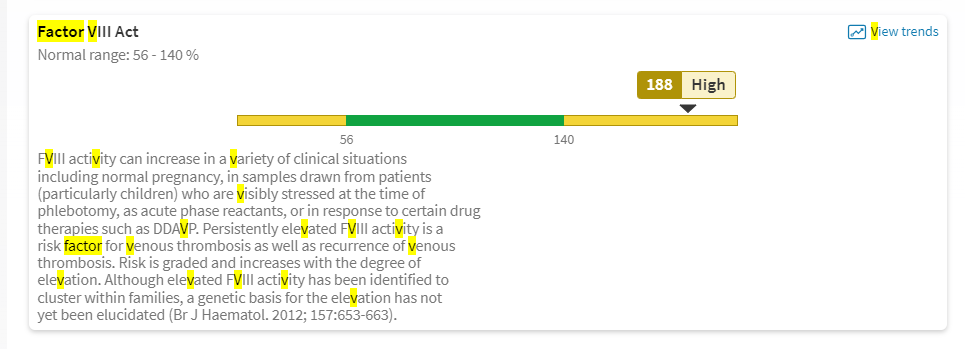
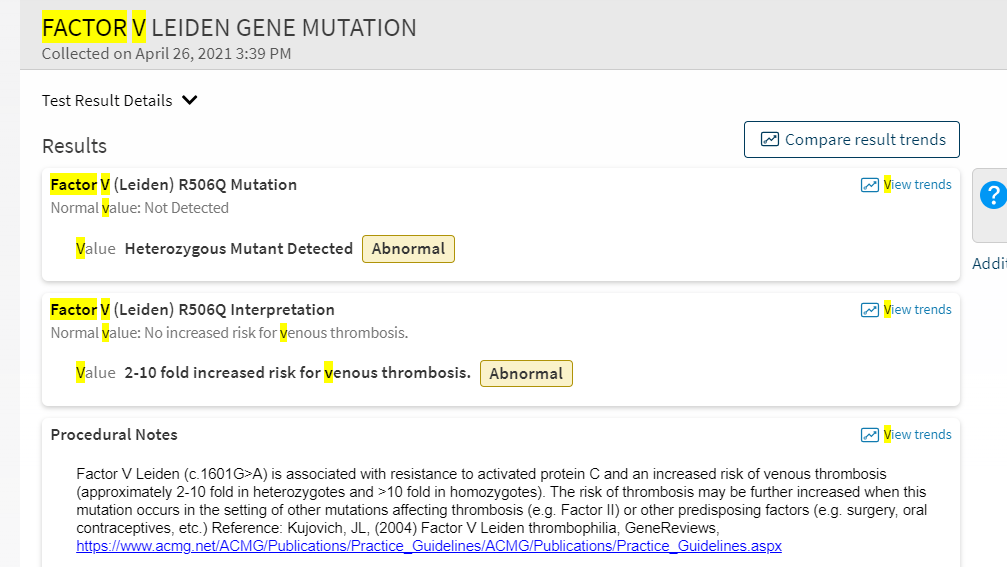
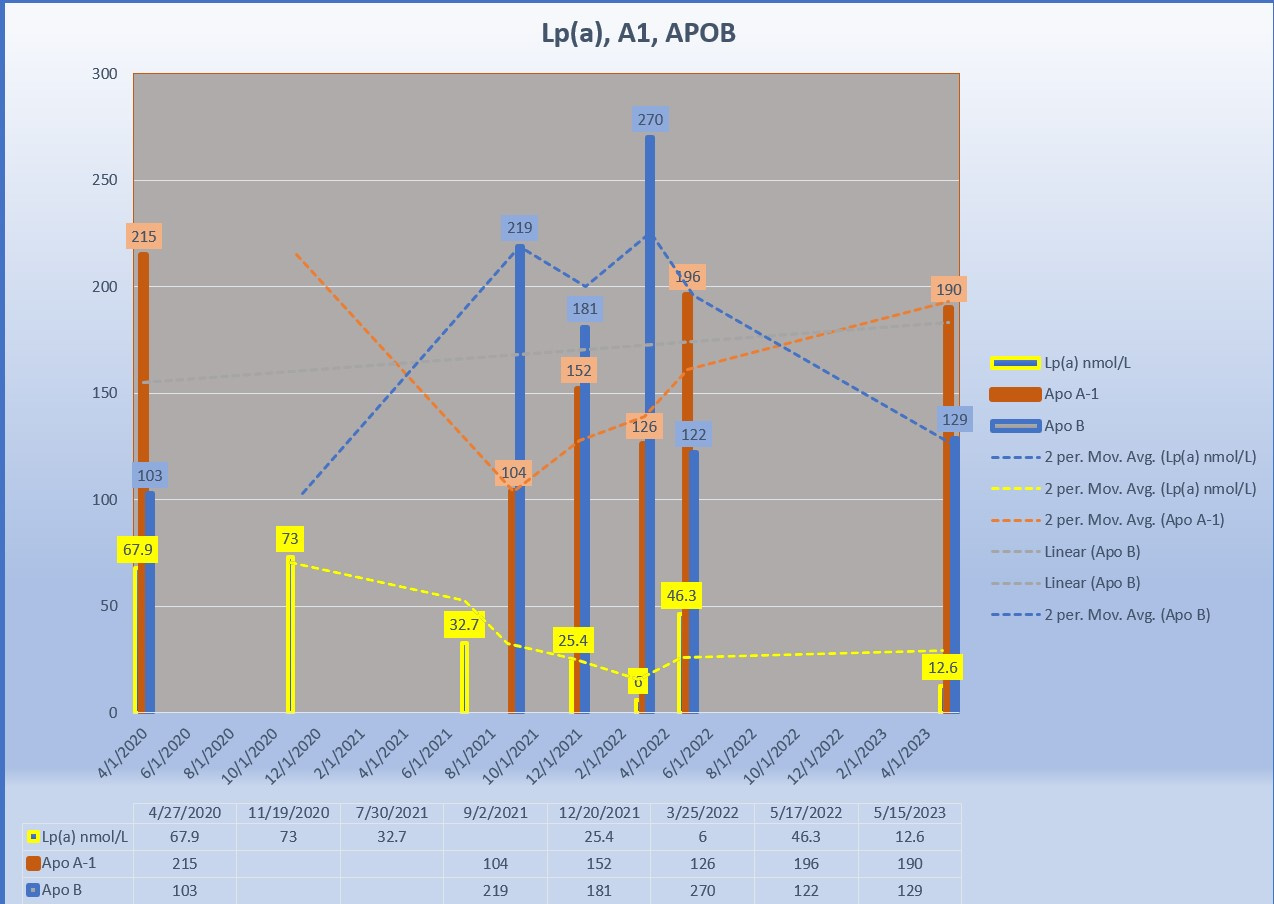
David Diamond gave a formidable presentation. He said outright that statins should not be used for LDL-C alone, his concern was Lp(a) and APOB. Especially if you have genetic predispositions for clotting . Afterwards I asked which genetic mutations and he told me FVIII. I asked how about FV and he was unaware if it was as damaging as FVIII. So then I said I have both, yay me!! to which we had two great discussions at different times about this, and I showed how I can manipulate both. This was worthy of his praise, and he encouraged me to continue my research into how I did this. I told him about a study I want to conduct and he encouraged me to do so. Even gave some advice on how to do it.
@Sodfather Presented a message that asked “How are you going about presenting LCHF?” and gave us ways to do so that might not be thought of. Stock local libraries. Visit your School Board. Utilize your counties Extension College and ask for help.

This was the first time I met Dom. What a gentleman and kind person. His wife Csilla is also very kind. I thanked him for his cancer work and how it helped my Herakles live 1400 days plus when his diagnosis was 550 days. We began to talk dogs and later that night when he learned of my wife’s Ehlers Danlos diagnosis, he sent me two links to papers his students have written for dissertations on their use of ketones in EDs. In person conferences are absolutely the best. So many other amazing stories to tell. His talk focused on all the NEW ways Ketones are being used as A DRUG, not just a metabolite
Chris from Keto Chow ( platinum sponsor!!) filmed it all and will edit this. I have no Idea when the Youtube’s will be out.