Someone is paying…. There are no drugs that cost $0 to produce, distribute and sell, however out of patent they may be. I would imagine that your government (ie the taxpayer) is paying?
I believe there are some statins that are now out of patent, and the drug industry is madly marketing the new statins to make sure their gravy train continues.
Simple, nothing is free. It all gets paid for by someone. If you get it for free then it’s probably coming from the health care providers who are being subsidized by your government who in turn are able to subsidize it with the taxes taken from you. So, it’s not free. You just don’t pay up front.
In America we pay the highest prices for medicines than any country I’m aware of.
Our neighbors to the north and south pay much lower prices but the pharmaceutical companies make up for the cost by charging us more. It’s no different than the hospital that treats a patient and the patient doesn’t pay the bill. The costs get passed on to those who will pay.
Statins in America are fairly inexpensive but with them being prescribed to nearly everyone these days who go to a doctor it’s a billion dollar industry.
Statins used to only be prescribed if your cholesterol was over 200. Then that threshold was dropped to 180. I believe it’s been lowered or suggested that 140 should be the new marker. Doctors are even suggesting that just as a matter of course that everyone should be on them, even children.
It doesn’t have to be expensive if it’s being mass marketed to everyone. It’s the Wally World business model of selling in volume allows for lower prices that equate to more profit.
The pharmaceutical companies and insurance companies control the medical community’s.
The argument that statin pushers make is that it is proven/obvious LDL causes CVD, and therefore any target level that does not decrease CVD in general is therefore too high, and therefore the target LDL level should be reduced until CVD in general is reduced.
The obvious problem here is the initial firm belief (because that is what it is). What does CVD history look like if LDL isn’t actually causal? Well, exactly what we’ve seen… increasingly prescribed statins successfully driving lower and lower average LDL levels in the general population, and increasing levels of CVD.
My conclusion from this evidence is that LDL is not causal. The medical authorities’ conclusion is that the LDL levels have not yet been driven low enough. I am placing a bet (my life) that I am right and they are wrong. Yes, it is that serious! With a current LDL level of 450 (it has always been very high) and a current CAC score of 10 (which is not zero, but is very low) at aged 60, thus far I am being proven right.
I have never taken statins, and I never will.
PaulL
(You've tried everything else; why not try bacon?)
#24
“For every complex problem there is an answer that is clear, simple, and wrong.”—H. L. Mencken
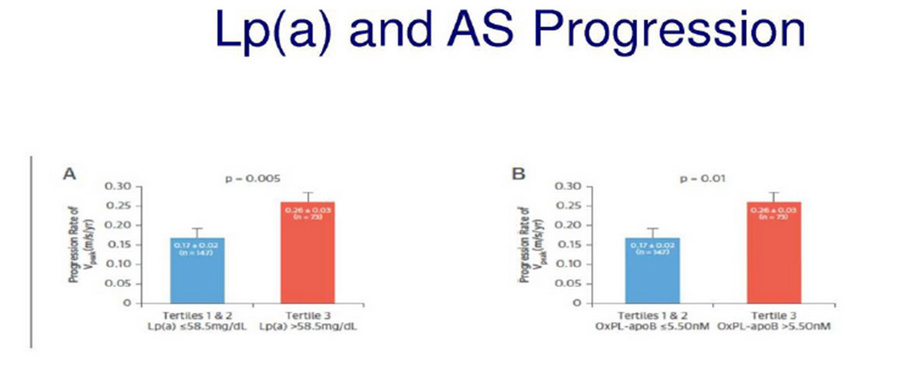
From the research I’ve seen (admittedly nowhere near Dr. Kendrick’s), there is a correlation between higher Lp(a) and higher atherosclerosis in certain instances. See this for instance (AS = aortic stenosis, which is basically calcification):
My Lp(a) levels, just for comparison, are above Tertile 3 by about DOUBLE that.
The issue is that I get a test every 1-2 years that measures aortic stenosis, and I don’t have that. I also have a zero score (as of a few years ago) on a CAC scan.
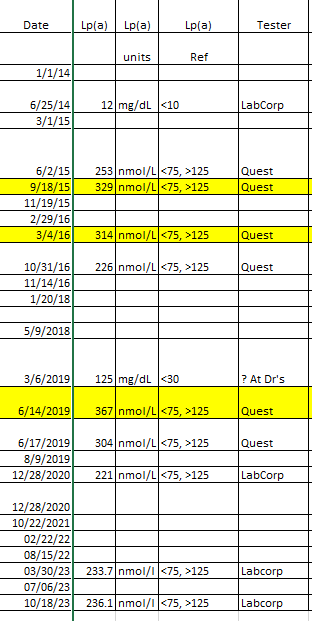
Here are my levels (yellow is after 4.5 days fasting, and LDL and Lp(a) levels go up during that time):
My theory therefore is that Lp(a) could be an “accelerant”, meaning if you’re getting aortic stenosis, higher Lp(a) could accelerate the process.
It’s still a tough issue, because my Lp(a) is so high that I’d need to drop my Lp(a) by a ridiculous amount. The smallest “normal” Lp(a) I have was 221 nmol/l, and the “good” range ends at 75 nmol/l. I would have to drop my Lp(a) by about 2/3 to get into that range. I do not know of any way to do this.
Another issue is that it could be the genetics that causes higher Lp(a) that is causative for some or all of this. Similar to FH (familial hypercholesterolemia), for instance, where some think FH is bad because of coagulation and not LDL, maybe the genetics that causes high Lp(a) causes something bad to happen?
There are drugs that are being tested to lower Lp(a):
My problem is that if I have no known ill effects from high Lp(a), why should I reduce my Lp(a)?
I got to 50:54 in the video but have to go do family stuff. I am glad he discussed ApoB, yet something else that’s considered to be deadly. I stopped listening to one of my favorite podcasts because one of the hosts said that ApoB CAUSED heart disease. He specifically said it was not correlated with heart disease, it CAUSED heart disease. Since I believed this not to be true, I had to stop listening to that podcast.
He said LDL cannot be causal in CVD because it cannot enter into the endothelium. Then he goes on to talk about the many ways the endothelium can be damaged… Oops, if it is damaged and the outer layer is stripped away, can’t LDL or oxLDL particles get into the “wound?” I would wager in the same time or even faster than Lp(a) can get there to form a scab. He only mentioned macrophages, but ignores them for the most part. Omission #2. He totally ignores the science showing that macrophages are always present in these plaques. That is known. They have been found there. They become what is called a foam cell, which is part of the inflammation process. So what are the mechanisms which can cause the endothelial damage? Well, he talked about HBP. He also talked about the importance of nitric oxide.If the ability to make nitric oxide is compromised, blood pressure will trend upwards. Higher blood pressure can damage the endothelial wall at stress points as he mentioned allowing the various blood-born particles into the endothelial layer - which is why it needs to be repaired. He may very well be right about the importance of Lp(a) in forming a scab to start the repair process, but that doesn’t really explain why CVD can become so severe. I believe the process to be multi-faceted, which is why it has not been explained yet. At best, he is just explaining a little piece of the puzzle, and ignoring a lot of known science.
PaulL
(You've tried everything else; why not try bacon?)
#28
It doesn’t surprise me. There is a strong correlation between the amount of bandages and sutures used in emergency rooms and the number of knife fights in the hospital’s catchment area. There is a very strong correlation between the number of firefighters in a community and the number of fires. We’d probably be a lot safer if we restricted bandage and suture sales and forced a hiring freeze at the Fire Department.
i know you know better, Bob. I’m not picking on you, but on the underlying logic of the whole lipid misunderstanding.
The other possible hypothesis is that increased aortic stenosis requires the body to produce more Lp(a). I wonder how they ruled that out?
The dialogue has gone something like this, since I was a child:
Researchers: Don’t eat saturated fat; it will give you a heart attack.
Other researchers: Are you kidding? Show us the data and a plausible mechanism.
Researchers: Did we say saturated fat? We meant cholesterol; it will give you a heart attack.
Other researchers: Show us the data and a plausible mechanism.
Researchers: Did we say cholesterol? We meant LDL-cholesterol; it will give you a heart attack.
Other researchers: But the data show otherwise.
Researchers: Did we say LDL? We meant Lp(a); it will give you a heart attack.
Other researchers: Show us the data and a plausible mechanism.
Researchers: Did we say Lp(a)? We meant oxidised Lp(a); it will give you a heart attack.
Paul
Yep, that is what I have seen, and alas, I think this dumb game will continue for a long time. There is too much at stake for certain interested parties.
PaulL
(You've tried everything else; why not try bacon?)
#30
Ravnskov and Diamond have posited that arterial damage occurs on a regular basis, but that under normal circumstances the body’s repair mechanisms can deal with it. It is when the damage occurs at too great a rate that we see plaque forming.
The crucial factor seems to be the coagulability of the blood. The difference between the people with familial hypercholesterolaemia who get cardiovascular disease and their relatives with equally high LDL who do not has been shown to lie in genetic irregularities that make their blood likelier to clot (primarily variants of fibrinogen and factor VIII). We’ve known that for sixty years.
We also know that a high-glucose (i.e., high-carbohydrate) diet promotes glycation of the haemoglobin, which in turn promotes greater coagulability. It also causes hyperinsulinaemia, which increases blood pressure and makes arteries more rigid, and thus more susceptible to damage.
But of course, it is the arterycloggingsaturatedfat that will kill us.
Just as a side note, though it may be my paranoia showing: All the doctors who were paid by the Sugar Research Foundation to pooh-pooh the dangers of sugar and to play up the dangers of saturated fat were good friends of Ancel Keys’s. Coincidence? One has to wonder.
Now, is high Lp(a) actually 70-90% genetic? I have no idea. It would take hours of research to figure that out.
And there are many other studies indicating that higher Lp(a) is “bad” for those who have certain atherosclerosis conditions.
But you bring up a good point about cause and effect. For instance (and maybe Dr. Kendrick refers to this later in the video), I’ve always thought that saturated fat does not “raise” “cholesterol”; instead, PUFAs (or maybe MUFAs) from plants “lower” “cholesterol”. I know Dr. Kendrick discusses how there’s no mechanism for saturated fat to raise “cholesterol”, because it gets packaged into cholymicrons, which don’t have a pathway to LDL. I believe the idea then is that sterols in plant-based oils lower cholesterol. Not sure if Dr. Kendrick discusses this.
But for me, the idea that saturated fat raises cholesterol is and always has been wrong. Saturated fat doesn’t do anything to “cholesterol”.
PaulL
(You've tried everything else; why not try bacon?)
#32
He sort of touches on it in passing. It’s Paul Mason who talks about this explicitly in his recent lectures. There is a mechanism (which I don’t remember clearly, but he describes it in some detail) by which phytosterols cause the body’s cholesterol level to drop. Then, when the person returns to a diet with healthier fats, the cholesterol rises, but it’s really returning to normal.
One of the main problems with cholesterol/Lp(a)/ApoB or whatever getting into the plaques is that the particles are found at the outside of the arterial wall, which means that, according to mainstream thinking, they somehow manage to pass through the entire arterial wall to get into place. It would make more sense if the particles passed into the arterial wall from the vasa vasorum, the network of blood vessels that supply oxygen to the arteries, as Dr. Kendrick mentions in the video. Ravnskov and Diamond have written a paper discussing this.
Coming from the vasa vasorum would mean that the particles are coming to strengthen the plaque from the outside, not somehow causing the plaque from the inside. Dr. Mason’s hypothesis, by the way, is that the crystal-shaped holes we see when plaque is stained for examining under a microscope could well be from phytosterols instead of cholesterol (whatever they are, they are apparently dissolved by the stain that is used). I’m not sure why that should be, or what it’s relevance is–plenty more to learn.
Well, I’m trying to get through this. He discussed homocysteine, high values of which are bad. Well, that’s another thing I have, is a relatively high value of homocysteine, because I am part MTHFR, which means I get higher values. Not excessively high, but higher. The main problem is that the studies I’ve seen where people lower homocysteine, there’s no benefit. But Dr. Kendrick was discussing very high levels of this, not what I have.
PaulL
(You've tried everything else; why not try bacon?)
#34
I suspect that, as with a lot of measurements, if we are eating an appropriate diet, our body can be left to manage itself, and out-of-range values aren’t necessarily a problem (though of course they might be). Especially when a lot of the “normal” ranges are calculated off an unwell general population.
I was astonished when I learnt this, and it just shows how far we have to go in the world of medical science. Right now, we have lots of tests for all sorts of things in the body, but we seem to not know what the optimal levels should be in healthy people. As far as I understand it, the reference ranges are simply averages of all the test results taken, regardless of the health condition of the patient source. Corrections to this understanding is most welcome.
Yes, that is my understanding. I am not sure how they define the limits, but it is based on a distribution curve of all of the population results.
PaulL
(You've tried everything else; why not try bacon?)
#38
I’m told that in the U.S., what most labs do is to take the range of the first 1000 supposedly well people through the door to take that particular test that year.
Here’s another video with Dr. Kendrick that talks about the diet-heart hypothesis and heart disease:
When I learned this I came to the conclusion that there is not a range that us carnivores can fit in therefore they are not a reliable metric for us.
Comparing my numbers against a population of people who primarily eat the SAD is like comparing the blood work between a canine and a bovine. It’s just not going to add up. Yeah I know that’s an example between to different species but you get the idea.
And another good one to watch. The doc is a cardiologist, and the other has a doctorate in habit change (?), and while not quite as important, she looks like my wife (hubba hubba )

 With a current LDL level of 450 (it has always been very high) and a current CAC score of 10 (which is not zero, but is very low) at aged 60, thus far I am being proven right.
With a current LDL level of 450 (it has always been very high) and a current CAC score of 10 (which is not zero, but is very low) at aged 60, thus far I am being proven right.

 )
)