This is a grab straight from the Australian Dietary Guidelines 2013.

I would avoid most of those other than processed meat too … but it’s not the Saturated fat.

This is a grab straight from the Australian Dietary Guidelines 2013.
I would avoid most of those other than processed meat too … but it’s not the Saturated fat.
@richard What do you think about this?
Asthma Foundation - Saturated Fat and Asthma
Do you know of any research that proves that saturated fat is more fattening than other fats or that it is inflammatory?
It has been found that for people with asthma, a diet high in fat is associated with an increase in the number of airway eosinophils1, whilst one high fat meal can result in airway swelling within hours2. Another study showed a direct link between the amount of hamburgers (a food typically high in saturated fat) eaten and asthma symptoms - the more hamburgers eaten, the more asthma symptoms3.
References:
None that I know of.
As I understand SFA is associated with cardiovascular disease when seen at high levels in circulation - note that is saturated fat in your blood not in your diet, but plenty of people who should know better conflate the two. Jeff Volek showed that people who are fat adapted and eat saturated fat have low levels in circulation because they preferentially use SFAs. People who overeat carbs make the excess into saturated fat would have high levels in circulation because they aren’t using any, and people who have insulin resistant fat cells that can no longer hold onto energy spill SFAs into circulation too. Those are all inflammation states - so SFA in the context of a high carb diet probably should be a concern.
I briefly looked at the abstracts and came away with a few obsevations.
Study #1:
Leptin levels were increased in both male and female asthmatics as compared with healthy controls.
…
It was found that asthmatics within the subgroup of severe persistent asthma have a different pattern of dietary intake as compared with healthy controls, which was associated with lower lung function and increased airway inflammation.
I’ll go out on a limb here, and say that leptin resistance is associated with insulin resistance, which is associated with SAD. The higher fat and less fiber reported in the food history surveys suggests consumption of high glycemic foods plus high(er) fat. Bad combination.
Leptin elevation stuff.
Study #2
Nonobese subjects with asthma were randomized to consume a high-fat (n = 19; 48% [49 g] fat) or low-fat (n = 18; 15% [3 g] fat) meal.
…
Changes in plasma fatty acids correlated with changes in sputum % neutrophils and were negatively associated with changes in % FEV(1), % FVC, and FEV(1)/FVC
…
Another group of patients with asthma consumed a high-trans (n = 5; 5.2 g trans fat) or nontrans (n = 5, <0.3 g trans fat) fatty acid meal. … After the high-trans fatty acid meal, sputum % neutrophils were significantly higher than after the nontrans meal.
What was the carb content and type? What was the insulin status of the test subjects? Insulin response (resistance) will indicate degree of fatty acid is uptake to adipose.
Plasma fatty acid fluctuations correlate with sputum. Interesting. I wonder what would happen during fasting when fatty acids are being mobilized from body fat instead of being ingested?
Yeah, trans fats bad.
Study #3
a cross-sectional prevalence study of 1321 children (mean age = 11.4 years, range: 10.1–12.5) was conducted in Hastings, New Zealand. Using standard questions we collected data on the prevalence of asthma and asthma symptoms, as well as food frequency data.
…
After adjusting for lifestyle factors, including other diet and BMI variables, compared with children who never ate hamburgers, we found an independent risk of hamburger consumption on having a history of wheeze…
Correlation with no other dietary information available. Did they have sugary drinks with those burgers?Again, most likely high fat and high glycemic, which is the worst combination.
Just thought of another possible link between fats and asthma. I was looking into a study about cream and endotoxins here. Maybe the connection is LPS and/or microbiome related? Part of leaky gut syndrome. Keto should help that because circulating BOHB protects the gut barrier. references to some studies here
Thanks for this info, Jamie Hayes. Is this pertaining to saturated fat or fat in general? What would you suggest one does if their asthma and allergies has flared up months into keto?
Eliminating saturated fats from your diet??
I’ve been on keto for the last 1-1/4 years, with no cheats. I closely track my macros and I thought I was right on the money. I feel great, BG, HbA1c, inflammation, etc. All good but cholesterol a bit high. I wasn’t worrying about it too much based on all I’ve heard,… Until my doctor was stressing about my LDL levels at 249. So I went to the guru! Then I became more concerned when I came across the following statement on Dave Feldman’s website, (cholesterolcode.com), especially knowing he’s a keto fan like me and seems to strongly promote the keto lifestyle.
Am I reading this right? Avoid saturated fats?? Yikes!
"Saturated Fats
Eliminating saturated fats from your diet will lower your atherogenic index and promote heart health when it’s part of an active lifestyle."
Fellow keto-folks, I really need your help on this!
I’ve been eating everything on the list, beef, pork, lamb, dairy products, poultry fat, cheeses, etc.!
Help! Have I been eating the wrong fats all this time while on keto?
Is there a typo on the site??
Best regards
Dave B
Keto and not budging, but I need some feedback urgently!
You might be able to lower your LDL some by swapping in more plant fats such as extra virgin olive oil, coconut oil, walnuts, pecans, avocados, etc. Vitamin B3 as nicotinic acid also lowers LDL. But it is debatable if lower LDL is healthier, especially if inflammation is low.
Just reading about fats and seeing that saturated fats from animals are in question with Gut Health and Endotoxins. This makes me question a lot. Have you had any luck with getting more information?
Some thoughts:
Ratios?
SCFA (pro-inflammatory?)
LCFA (anti-inflammatory?)
Or is it deeper than that?
Type and condition of fat/oil fresh or rancid (oxidized) used; e.g. extraction process; pressed, virgin, extra virgin or processed; heated\thermal conditions i.e. not stepped on? …and is it ORGANIC?
Cooking: Heated? What temperatures\thermal conditions? What happens to it?
Thinking in hunter-gatherer-terms; in the very beginning they may not have been doing a lot of gathering (storing) if they were on foot and highly mobile; nomadic; they did not have time to store a lot of things!
Formation of short chain fatty acids by the gut microbiota and their impact on human metabolism Short chain fatty acids (SCFA) are the primary end-products of fermentation of non-digestible carbohydrates (NDC) that become available to the gut microbiota. They represent the major flow of carbon from the diet, through the microbiome to the host.
Are Short Chain Fatty Acids in Gut Microbiota Defensive Players for Inflammation and Atherosclerosis? Conclusion and Perspectives
SCFAs may suppress inflammation by reducing migration and proliferation of immune cells, reducing many types of cytokines, and inducing apoptosis. Thus, SCFAs are thought to have anti-inflammatory effects. However, marked changes of SCFAs concentrations in blood or various tissues are thought to cause disorders related to immunological and metabolic imbalances. Thus, gut bacteria exert both beneficial and harmful effects107. Therefore, it may be important to estimate the appropriate concentrations of SCFAs to maintain a normal metabolism and immune system for the prevention and treatment of diseases using diet and SCFAs. Recently, Bergeron et al. demonstrated that a lower carbohydrate diet (39–40% energy) high in resistant starches was associated with higher plasma TMAO levels in spite of reduced postprandial insulin and glucose responses, while there was no difference in TMAO affected by resistant starches when carbohydrate intake was high (51–53% energy)108). It may be necessary to develop food patterns or medications to reduce plasma TMAO concentrations and maintain appropriate concentrations of SCFAs.
Although there have been only a small number of studies thus far, in the future SCFAs may provide new insights into the pathophysiology of inflammatory diseases, and we can expect the development of novel therapeutic strategies against chronic inflammation, metabolic disorders, and atherosclerosis.
Short, but Smart: SCFAs Train T Cells in the Gut to Fight Autoimmunity in the Brain Abstract In this issue of Immunity, Haghikia and colleagues (2015) demonstrate that dietary fatty acids, by modulating gut microbes and their metabolism, regulate mucosal immune cells to impact systemic immunity. Using this mechanism, dietary and bacteria-derived medium-chain and long-chain fatty acids exacerbate, whereas short-chain fatty acids ameliorate, autoimmunity in the brain.
Gut Microbiota and Metabolic Health: The Potential Beneficial Effects of a Medium Chain Triglyceride Diet in Obese Individuals 5. Synthesis and Conclusions
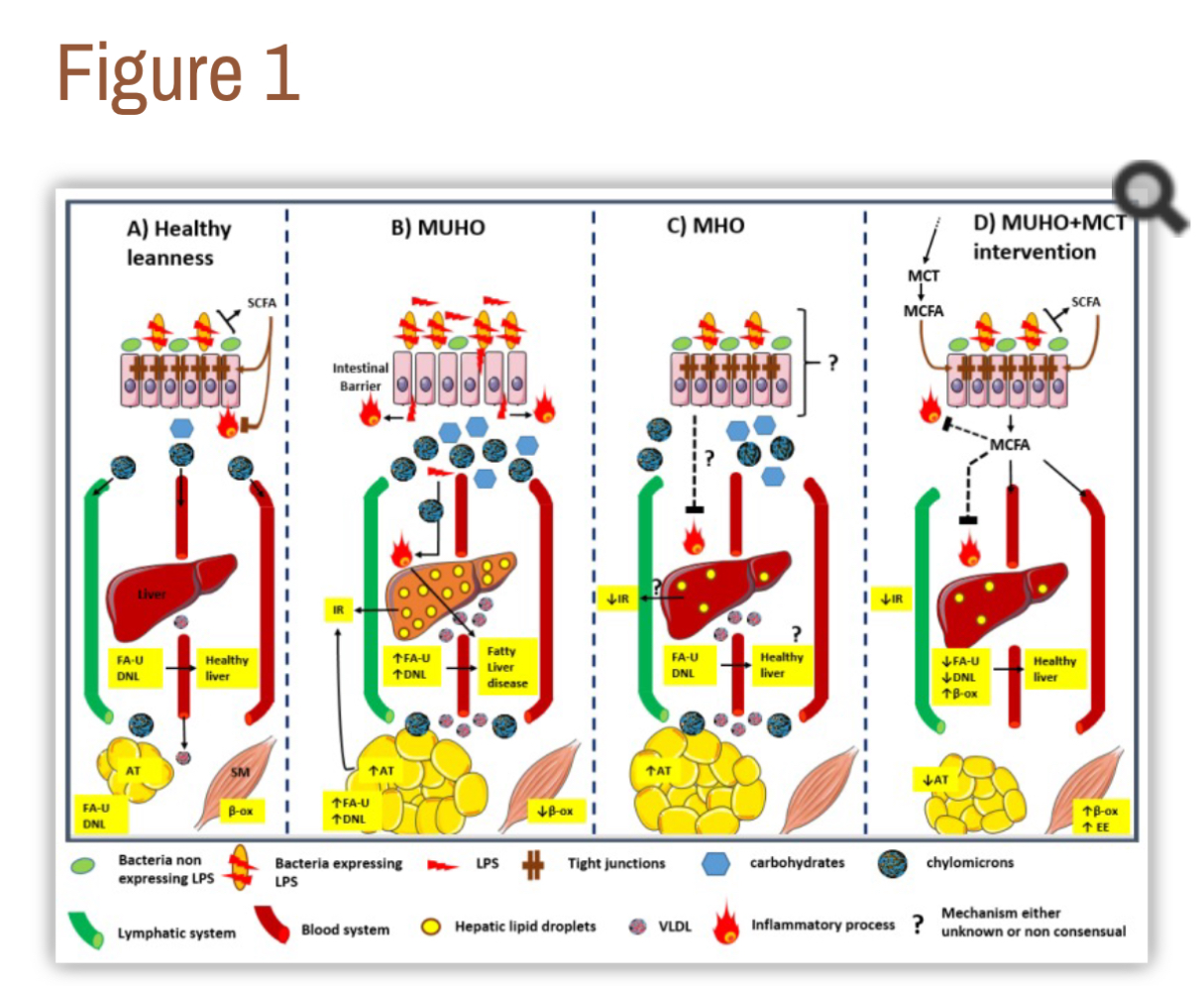
This review aimed to highlight several aspects underlying the condition of obese subjects, which can be either metabolically unhealthy obese (MUHO) or metabolically healthy obese (MHO). While a panel of criteria serves to define the MUHO state, those defining metabolically healthy obesity remain the subject of current discussions. We underline the necessity of better defining the potential role of gut microbiota in the establishment of MUHO or MHO states. Moreover, we believe that gut microbiota structure may not only serve as a biomarker of those metabolic states, but can also be subjected to a diet-induced remodelling, modifying in turn the metabolic status of patients (MUHO vs. MHO or lean state). Dietary MCT, taken alone or with other supplements (such as prebiotics, probiotics, organic acids, etc.) could be used as anti-obesity interventions, in regards to their capacity to prevent intestinal permeability/endotoxemia by remodeling gut microbiota, and to prevent unhealthy storage by improving the lipid catabolism/anabolism balance. Figure 1 illustrates this concept.
Saturated Long Chain Fatty acids Activate Inflammatory Signaling in Astrocytes
Metabolism meets immunity: The role of free fatty acid receptors in the immune system
Dietary fatty acids and susceptibility to multiple sclerosis
You need to show exactly where this quote is. I searched his site and couldn’t match even a subset of that phrase. Are you sure you didn’t get it from the comments?
It sounds highly improbable given what we know about science and @DaveKeto and reads like a soundbite from the recent AHA BS about saturated fat that Dave did comment on (unfavorably).
I wrote Dave immediately after I found this embedded in his site in the Cholesterol “Report tool”. I believe it was pasted in as a piece of another article on his site.Ilanded on it from the Cholesterol risk assessment Tool section. I just checked and it’s still there…
Not sure why.
I’m not panicking in any case. Still loving my juicy ribeyes.
Regards
Dave
It’s BS, written by some unqualified bro, taking stuff from the AHA and mashing up some other sources. He knows that HDL:Trigs is the best ratio to test but then spews some AHA BS about saturated fats… when we know from thousands of people here that HDL goes up and trigs go down on a saturated fat diet. If anything goes up, it’s LDL and that doesn’t much matter.
Ignore and go about your business. Nothing to see here.
(It is weird that the link is still there).
Okay – I see what happened. You followed the link that I have for an article on Atherogenic Index of Plasma. The report page that gives this link is here: http://cholesterolcode.com/report/ and the article itself is here: http://www.safehealthmedicine.net/atherogenic-index-heart-disease-predictor.html
So I don’t control that conclusion the author comes to, I was mainly wanting people to be able to dig deeper into what the AIP is and how it is calculated.
That said – the VAST MAJORITY of people who follow my site have the lowest category of AIP risk while downing lots and lots of saturated fat. So you can come to your own conclusion on how accurate this statement is for yourself.