I had to pause, there, and feel the universe wobbling. "Wait a minute - this dude’s name is actually ‘Hyperlipid’?" Okay, so Peter Dobromylskyj – Hyperlipid - this came up right away when I searched, and looks like a righteous bloke, but I did have to laugh.
PaulL
(You've tried everything else; why not try bacon?)
#34
He is (or was) a veterinary anaesthetist by profession, but he’s one sharp cookie. He knows how to read a study and has an excellent grasp of statistics. I don’t always understand his posts, but I trust his objectivity and commitment to following the data wherever they lead.
We still need to be able to separate the wheat* from the chaff. (So to speak. )
Critical thinking reveals a good bit of what I said, immediately. ‘Pay-to-publish,’ etc. It can also be seen - literally in seconds, by scrolling down through the article - that there’s no peer-review, no qualifications given for the authors, they don’t even bother making claims about their education…
Respectable, serious science isn’t usually going to be that way, so the BS detectors and warnings about “stupid stuff” should be going off in our heads - that’s really all I’m saying. There is a LOT of lame stuff out there.
*Sorry for the mention of wheat, if anybody was offended.
No ketonians (and only 3 carbfiends) were harmed in the making of this post.
My naive understanding is that each person promoting and/or following a ketogenic lifestyle has a slightly different reason to do so and possibly a different appreciation of the mechanisms by which a miracle weight loss could occur. That might be the case for researchers too.
I have read the article and, just reading it, I could not see any distinction between having achieved ketosis or not in the studies allegedly debunking the carb-insulin hypothesis (I have not read the cited studies themselves in detail though). Still, the fact that being in ketosis or not does not seem to matter to the authors of the article doesn’t seem a good sign (the word ketosis doesn’t even appear once).
Even so, some questions are still worth asking: Hall et al paper (Ref. [12]) reports some interesting results with a larger weight loss for participants with higher fat intakes but a reported lower fat loss for the same cohort with high fat diet. Now, I am playing naive but I would a priori be cautious on how fat mass is being measured. I am happy to trust a weighing scale but not so much an estimate of the fat loss over the course of 6 days. Hall et al. use the DXA method which is not devoid of error (https://weightology.net/the-pitfalls-of-body-fat-measurement-part-6-dexa/) in particular from the hydration levels of the fat-free mass. Given a drastic change in diet over 6 days, it is possible that hydration levels of the cohort populations have been out of whack.
In general, my naive understanding of the “keto” hypothesis was not to follow calories but to follow instead fat. This could be summarised in an equation of the form:
dF = f(FI - FC) + g(CI - CC) where
FI = Fat in
FC = Fat converted
dF = fat mass variation
f = fraction of fat surplus/deficit which can be stored/burnt
g = fraction of carbs surplus/deficit which can stored/burnt
CI = Carb intake
CC = carb converted
In a ketogenic diet gCI ends up being ridiculously small compared to all the other terms so I will discount it for now.
FC accounts for fats being burnt and being converted for other uses in the body. The fat burning part is dictated by the energy expenditure which can be increased by physical exercise and various forms of intermittent fasting.
The factor f is mostly set by insulin levels.
With the simplistic equation above fat loss occurs if FI is less than FC i.e. if the mass of fat intake is less than the mass of fat needed to run the body.
A typical ketogenic diet has about 80% of caloric intake coming from fat. Assuming a similar energy conversion factor for dietary fat and stored fat we get that fat loss occurs if
Cal In < (BMR)/0.8
For an assumed BMR at 1700 Cals this gives that weight loss can occur if Cal In is less than 2125 Cals.
Of course the model above is simplistic and doesn’t even look at protein intake but it should not be too bad to give a heuristic rationale for why people in ketosis can lose weight even if they consume above their BMR.
Given that many people here are much more knowledgeable than I am on the matter, any improvement to the above stupid model are welcome.
Note that when I derived that Cal In < (BMR)/0.8, I assumed that all the energy required to run the body would be obtained from fat which is not true even for an optimum state of ketosis.
It is also noteworthy that when looking at mass fat balance, it can usually be converted into an equation with calories in and calories out under simplifying assumptions, except that there are some prefactors coming in.
A less radical take on CICO that would simply posit the necessity of an inequality of the form
Cal In < function(Cal Out)
as a requirement for fat loss (and where the function depends on the current metabolic state of the individual and, possibly, their diet) would not be incompatible with most of the narratives put forward to promote a ketogenic life style.
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#39
@Fabien_Paillusson Finally! Someone got past being silly over Bompa Institute. Thank you, Fabien.
Hall’s study is, indeed, a serious attempted rebuttal of the carbohydrate-insulin hypothesis. I link it below. Michael Eades has an excellent commentary on Kevin Hall’s claimed debunking of the carbohydrate-insulin hypothesis of obesity. Not a long article and well worth the read:
Hall’s study cited in the OP as discussed by Eades:
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#40
@anon81060937 Thank you for this article link! Please post the link here:
Hi Fabien. Very good post. Yes, there are several things like that. There is a big problem with a lot of studies that talk about “low carbohydrate” because they don’t go low enough for ketosis, or even as low as most people who want to “eat keto” aim for. So much of the “low-carb advantage” deals with insulin resistance - so to give it a fair test the people need to eat VERY low carb, so as to make a noticeable difference in their insulin levels. Then the results will be more on the side of the carb-insulin hypothesis. The degree to which the test subjects are insulin-resistant obviously would also significantly affect things.
DEXA scans may be fooled by different hydration levels in tissue. Water is a little “heavier” than our bodies, and if a DEXA scan “sees” more water in fat or nonfat tissue, it doesn’t know what it’s looking at, which can make a substantial difference. Hydration levels need to be controlled for.
You mentioned "Hall et al paper (Ref. [12])." Kevin Hall seems to want to deny the carbohydrate-insulin-hypothesis, from the beginning. Dr. Jason Fung gave a good critique and rebuttal about that study. Hall really did not give “low-carb” a fair trial.
This is a good subject, and I hope lots of people comment. More to come (I just don’t have time now).
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#42
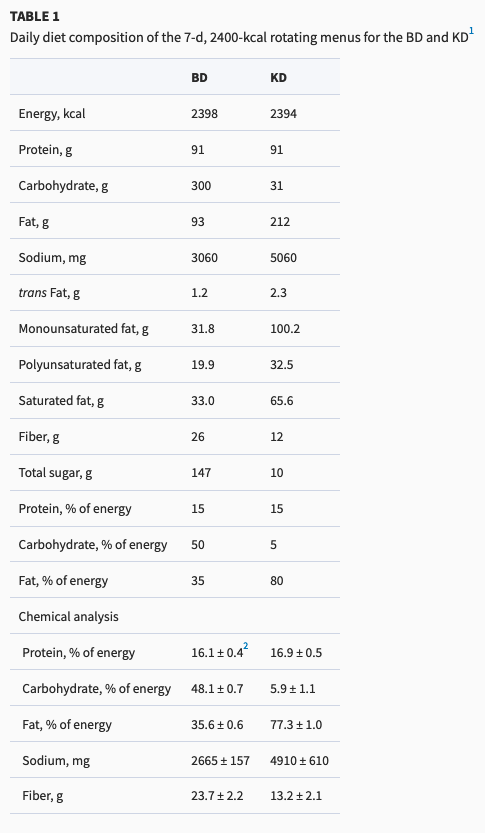
@OldDoug Following is the food content of Hall’s study, KD is the ketogenic version. I don’t think you can criticize this as not low enough for ketosis. It likely was for most if not all subjects. Read Eades’ comment on the study. According to Eades the real problem (for Hall) is that the study confirms keto rather than not.
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#43
Fung’s critique of Hall’s study. Like Eades, Fung suspects that the findings of the study didn’t support Hall’s wishful thinking so Hall just made up what he wanted.
You can if you want but those effects only apply on a carbohydrate diet. Something else happens when ketogenic but not in everyone who is ketogenic for various reasons.
What causes obesity isn’t directly insulin but the indirect “search” for blissfulness. The more someone eats carbs… the more their serotonin and probably other neurochemicals rise but never enough to make them feel blissful. Then not eating carbs will lead to a drop in Serotonin. Vicious cycle of addiction. Insulin is just a bystander.
Okay, yeah, makes sense. I wasn’t referring to Hall’s study but rather a generalized view of purported “low-carb” studies, which sometimes means “only” 15% or 25% or even 40+% carbs.
So, 7 day rotating menus? That sounds brutally insufficiently short, to start with. Again, not specifically about Hall’s study, since I don’t know the details offhand, but somewhere in this thread is a mention of studying people where they ate varying diets for 4 weeks, then an equalization or ‘washout’ period, and then 4 weeks of another diet (high or ‘low-carb’) it was claimed. But even 4 weeks really is not enough to give true low-carb a fair trial, i.e. fat-adaption alone can take longer than that.
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#46
@OldDoug I agree that most studies that find ‘ketogenic diets don’t work’ are either of too short duration and/or too high carb meals that are portrayed as ‘low carb’ or ‘ketogenic’ when not. I suspect that if Hall’s study had been longer it would have shown even greater fat loss than it did. But even at only 4 weeks, it showed fairly conclusively that the KD diet works. Both Eades and Fung in their independent analyses agreed the data showed a positive result from KD. Both also agreed that the data not only showed a positive KD outcome, but so positive an outcome that Hall had to spin the results with bafflegab to try to make it look bad.
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#47
One issue that Eades discusses is the metabolic chamber in Hall’s study:
But immediately Hall tells us there was something wrong with using the metabolic chamber. As Hall says, much to their surprise, they found out that the energy expenditure of subjects in the chamber is unnaturally low. So when the researchers fed the subjects the number of calories they thought they needed as revealed by the metabolic chamber they were dramatically underfeeding them. There was quite a discrepancy. Says Hall:
One of the interesting things was that despite the fact that we were trying to put them in energy balance in the chamber and we were actually able to do that. Um, outside the chamber they actually burned more calories. Not too surprising in retrospect but we actually were surprised by the magnitude of how many more calories they were burning outside the chambers. Upwards of 500 calories a day more outside of the chamber than inside the chamber. So what that meant was that we were feeding them more or less in balance in the chamber but we were underfeeding them outside the chamber.
When Hall says, “not too surprising in retrospect,” he might as well be saying “oops!” And what he also means when he says that is his own colleague and last listed author on this study, Eric Ravussin, published this finding 25 years ago. This makes me wonder why they didn’t plan for it in advance.
Here’s the full text (pdf) of the study that Hall and Ravussin published 25 years ago that Eades finds interesting. Here’s a more recent paper discussing the same phenomenon, ie subjects expend much more energy on the metabolic ward than in the chamber.
In Hall’s study, the people consumed from 31.1 to 40.5 grams per day for the ‘ketogenic diet’ phase. Insulin did decline, and ketones increased by a factor of ~7. For Beta–hydroxybutyrate, the average level was 0.758 mmol/L, so not far into ketosis at all, really just toward the lower end of “nutritional ketosis.”
This does seem to be the case, and to what extent could Hall’s study truly “debunk the carb-insulin hypothesis”? The write-up of the study begins with this sentence:
The carbohydrate–insulin model of obesity posits that habitual consumption of a high-carbohydrate diet sequesters fat within adipose tissue because of hyperinsulinemia and results in adaptive suppression of energy expenditure.
(Just on its own, that doesn’t seem quite right to me. High-carbs; fat storage because of high insulin = all good so far. But to say that “results in adaptive suppression of energy expenditure”? I don’t see it as a necessary “adaptation,” but rather a different description of the same thing. Energy being stored as fat means that it’s not available for metabolization, for expenditure.
So by definition at that point there is less available energy for expenditure; considering the energy balance demands acknowledging that. Thus it’s not that the body “decides to expend less energy,” i.e. adapts in that way, it’s that it has no choice.)
More importantly, I think, the carbohydrate–insulin model (CHO) doesn’t claim that everybody who eats high-carb will suffer the same metabolic fate. CHO says it can happen. It does happen for many people. But just because a given group of people don’t display a marked difference when on different diets does not mean that CHO isn’t valid for others.
Nor that advantage for low-carb would not become more apparent under different conditions and/or longer time periods. The study participants were said to be “overweight or obese,” so I’d assume there was some insulin resistance there, but it’s a question as to how much.
Low-carb resulted in “Daily insulin secretion, as estimated by 24-h urinary C-peptide excretion, rapidly and persistently decreased by 47%…” It would be nice to know what the fasting insulin levels were, at the beginning of the study and at intervals along the way. Insulin went down, as one would expect it would, but we’re left hanging as to just how insulin-resistant the subjects really were.
The test subjects were really not used to ‘eating keto.’ People whose habitual diets got less than 30% of calories from carbs were rejected. 4 weeks on ‘low-carb’ is not long enough to get an accurate picture. If they aren’t fat-adapted, then energy expenditure will very likely be less, resulting in interpretations that CHO isn’t doing what it claims to do.
I’m thinking this could skew things. 4 weeks on baseline diet, then 4 weeks low-carb. If less water retention - as is common - resulted from the low-carb phase, then this would be a confounding factor (actually making CHO look better).
Yes, and thus ‘f’ (which as you say is mostly set by insulin levels) becomes exceedingly important.
Kevin Hall is no defense for the Tudor Bompa Institute, nor vice-versa.
Consider a person fasting for more than a day or two - long enough for glycogen to be essentially “used up,” as much as it can be. Things get fairly simple indeed then.
PaulL
(You've tried everything else; why not try bacon?)
#50
Does it actually get used up, or does the body start to make more from scavanged protein (autophagy and gluconeogenesis)? Do we even know?
This is a fascinating discussion. Thanks, all, for your thoughtful contributions.
It makes more. There’s still parts of the body that have to have glucose, so some of that is going around, and even with ultramarathoners and the like there’s still some glycogen that will be there (after exercise-induced depletion), though likely only a tiny bit. Just a guess - we know the body will be eventually very reluctant with fat as starvation progresses, it doesn’t want to give up that fat and risk truly having the tank run empty and dying. For glycogen I’m thinking of it like it’s exponential - it goes down but as it nears zero the rate of depletion also slows down a lot.
For people who fast, being on a very low-carb diet when eating means a slower rate of glycogen production. I assume it’s far less than on high-carb. I picture it like for extreme long-exercise athletes. Fasting means even less glycogen production, but over time the body gets used to that happening and compensates.
For that matter, I’m guessing it’s that way for high-carb diets too. First couple times fasting, maybe the body thinks it’s just a momentary hiccup in the food intake and that lots more carbs will soon be in the pipeline and it will be easy to replenish glycogen. But with a lot of time fasting, the body learns and adapts…?
I think, that 31g carbs is too high for the KD / ketosis diet, and furthermore, KD is way too high in the unhealthy polyunsaturated fats. 33% of the 31g of carbs are sugar; this also is a no-no. 91g of protein, if we allow 0.7g protein x LBM (lbs), then this diet, I suppose, is referencing a diet made for a person with a LBM of 130 lbs. If we use 0.8g protein per LBM, then the body LBM weight would be around 114 lbs.


 I had to pause, there, and feel the universe wobbling. "Wait a minute - this dude’s name is actually ‘Hyperlipid’?" Okay, so Peter Dobromylskyj – Hyperlipid - this came up right away when I searched, and looks like a righteous bloke, but I did have to laugh.
I had to pause, there, and feel the universe wobbling. "Wait a minute - this dude’s name is actually ‘Hyperlipid’?" Okay, so Peter Dobromylskyj – Hyperlipid - this came up right away when I searched, and looks like a righteous bloke, but I did have to laugh.