
How much we need for gng? I’ve read various numbers before… Let’s say I eat 15g carbs on my carnivore-ish woe (I usually get usually 5-20g from animal sources), net is almost exactly the same as total and I am fat adapted since long. How much glucose my brain needs? Not much, I know that but still… 50g in total so another 35g? I’ve read that number once. Or no one knows because there is too much differences between people? Is it one of the zillion cases where one just should listen to their body as long as it’s a smart body with good communicating skills? Still, I guess there is some estimation. Our protein need usually isn’t nearly as big a mystery as many other things in our woe.
What do you all think of this article about meat and insulin?
PaulL
(You've tried everything else; why not try bacon?)
#27
Not necessarily, but there is a certain irreducible daily nitrogen loss, of which gluconeogenesis is certainly a part, when it’s happening. That’s all I meant.
Protein is our only source of usable nitrogen; we can’t take it directly from the atmosphere. I suspect that if it weren’t for that, the anti-meat forces would have excluded meat entirely from the food pyramid.
Lc14503
(Laura)
#28
Might there be a difference for processed vs unprocessed meats? (Even if processed have no added sugar)
PaulL
(You've tried everything else; why not try bacon?)
#29
Gluconeogenesis is not the only reason we lose nitrogen. The body also uses nitrogen oxide for regulating blood pressure (and insulin interferes with it, which is why hypertension is one of the chronic metabolic diseases). Furthermore, the body has a limited capacity to store amino acids, and one of the ways to deal with an excess is to deaminate those amino acids and turn the liberated nitrogen into uric acid for excretion, if there’s no need for it elsewhere in the body. (Likewise, the deaminated amino acids can be turned into glucose or fatty acids, if needed.)
In any case, whatever is going on, we lose a certain irreducible amount of nitrogen every day, which is one of the reasons we need a certain amount of protein every day, since fat and carbohydrate don’t contain any nitrogen (only amino acids do). The classic study of the subject determined that the average nitrogen loss over the people studied was 0.6 g/kg LBM/day, so the daily recommendation was set at 0.8 g/kg/day to be safe.
As for gluconeogenesis, my understanding is that the liver makes a certain amount of glucose, when needed, and stores it in the form of glycogen. When there is a sudden demand for glucose, that glycogen gets sent out to the muscles, and the liver makes more. Unlike the skeletal muscles, the liver can share its glycogen, whereas muscles can dispose of the glycogen they make only by metabolising it. The old fear that the liver automatically converts all excess protein into serum glucose has been discredited, I believe.
PaulL
(You've tried everything else; why not try bacon?)
#30
That’s a good question. But so far as I know, the body doesn’t see “meat” or “protein,” it sees amino acids. Part of the digestive process is to break down proteins into their constituent amino acids, just as it breaks down carbohydrates into their constituent glucose molecules.
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#31
At this point it’s just an observation/hypothesis on my part. Many folks do, indeed, experience a ‘drop in ketones’ when eating higher protein. That’s not a myth. As you note initially this was thought to be a result of gluconeogenesis ramping up to convert the ‘excess’ protein to glucose. This can be tested by anyone with a CGM simply by eating a big protein meal and watch what happens to glucose afterwards.
My hypothesis is rather that the protein stimulates insulin which in turn inhibits ketosis. This could also be tested - indirectly - by anyone with a CGM. Eat a big protein meal and increased insulin should show up as a reduction of glucose.
Another interesting experiment to try would be to increase protein, but over the course of the day by small amounts rather than eating large ‘protein meals’. It would be interesting to see what happens to the glucose plot when you feed an ‘excess’ amount of protein, but slowly. Might not have the same affect on insulin rise. Maybe not inhibit ketosis.
ctviggen
(Bob M)
#32
My CGM showed zero blood sugar increase or decrease with massive amounts of protein per meal: 160g+, 200g+ / meal, as examples.
The issue is that you’re not considering glucagon. Insulin goes up, and this might drive blood sugar lower. But glucagon rises to counteract that. I’ve even seen theories saying glucagon was meant to be the dominant hormone, not insulin. Our blood sugars were primarily supposed to be raised by glucagon, not lowered by insulin.
I’ve also tried to test the whole “high protein = lower ketones” theory. I could never adequately test it. Sometimes, I thought it was true; other times, I had opposite results.
Also, ever since I saw this graph from a continuous BHB monitoring system, I knew I couldn’t test BHB anymore:
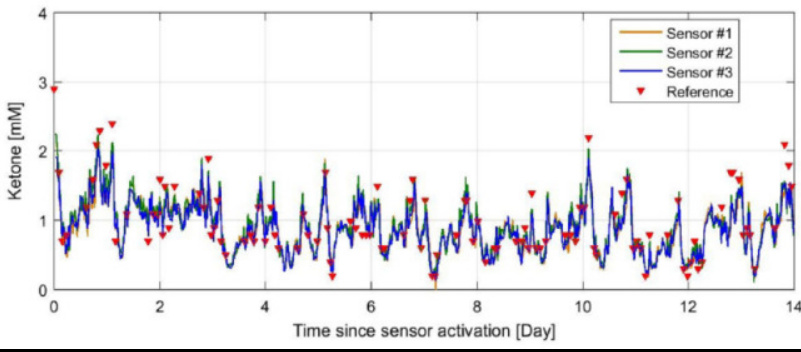
When your BHB levels look like that, pinprick testing doesn’t tell you anything.
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#33
Thanks, Bob. Yeah, without glucagon in the mix we’re limited in just what we can determine. I don’t think there’s a glucagon home device. So I thought next best thing was to see what we might infer from glucose readings. You seem to have already done the experiment and demonstrated the hypothesis wrong. I am soon going to buy another sensor for my FreeStyle and do this myself.
As for ketone measurements - any of them - my experience is also that they’re all over the map. As per the graph you posted above, individual data points don’t show much other than wide ranging variability, but I think if you plot the averages over time you may bet a useful daily plot, like with a CGM for glucose. It sure would be nice if we had a home CKM! When I was testing BRace multiple times per day I graphed some days into an averaged plot and that looked more useful than the individual data points.
‘Chasing ketones’ is like trying to smooth the variability at the top end. Whereas I think maintaining a relatively smooth curve is like more important - ie, like glucose, the more uniform the plot the better. Although I doubt we could ‘flat line’ ketones.
PaulL
(You've tried everything else; why not try bacon?)
#34
A drop in ketones, yes; but I haven’t heard of a rise in serum glucose. Or, rather, I thought that idea had been shown to be erroneous.
Protein in a low-carb diet has been shown by Bikman’s team to stimulate a rise in glucagon, which counteracts the insulin and keeps the insulin/glucagon ratio low. Or so I understand; did I misinterpret his lectures?
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#35
Unfortunately, I can’t measure glucagon so have no idea what it’s doing if I eat high protein, high fat or whatever. I’m not willing to do a high carb trial!
My bottom line is trying to determine why after 4 1/2 years on keto my ketones, at least BRace measured by my Ketonix, are in the basement. Saying this is ‘normal’ does not explain why/how it happens. I often say “A brain on ketones is a healthy brain”, but are brain ketones independent of ‘low ketone measurements’. Maybe studies that show protein raises insulin have been done exclusively with people eating some variation of SAD. Maybe Bikman is the only guy looking at the same with people eating keto. I would like to think Bikman is right, but something is driving down my ketones - and others’ ketones as well. I’d like to understand the mechanism. Glucose, insulin and glucagon seem to be the prime candidates for controlling ketone synthesis. Or maybe there’s an additional ‘Factor X’?
I don’t know, but I’m trying to find out. Right now I am trying a slightly lower protein macro to see what if anything happens.
Or maybe our brains are making their own.
ctviggen
(Bob M)
#36
I agree with you about the low ketones. Once mine got to 0.1-0.2 mmol/l every morning, I gave up measuring them. They did get higher if I measured at night, but if you’re trying to see if protein affects things, well if you’re near zero, you’re near zero. And – if “ketosis” is defined as any ketones – I never got “kicked out of ketosis” by protein.
I would like to know why only some of us get really low ketones. I believe Amber O’Hearn still has relatively high ketones, as in 1.0 or greater at times in the morning. Why does she have higher ketones, and we don’t?
I hypothesize it’s partly due to exercise. I think exercise can cause lower ketones, due to FFA usage. We switch over to that instead (let’s ignore the brain for now, and just talk muscles). To me, this means fewer ketones are needed. Maybe we are exercising more than the others who have higher ketones?
But, like you, I wonder about the heart and the brain. For my condition (cardiomyopathy), this is a type of heart “failure”. I’ve seen tons of evidence that the failing heart likes ketones. But what happens when your ketones are very low? Does the heart switch to FFAs over time? I assume so, but can’t find any good studies on this.
As for the brain, I have no idea how that works. While I still produce glucose, I don’t know how much of that goes to the brain and what the brain ends up using.
Naghite
(Michael)
#37
Hi Paul,
My understanding from Bikman’s lecture, was that in healthy people in a very low carb state, you are correct that insulin to glucagon ration stayed almost the same (rose slightly). The ratio would apparently fall if in a fasted state (I hope!). I am not sure if he was only looking at metabolically healthy individuals or not. I can say that when I wore my CGM, I could eat a meal of bacon and eggs and I could see a serum increase of about 1 mmol/L over the next hour or two. I may be different as a T2D however. While wearing my CGM I typically ate a few carbs (usually under 7) with each meal, and always saw this effect regardless of the time of day - although I am not sure I ever had zero carbs late at night while wearing the device. It is possible this was coincidence at the time – I have two more 10 day CGM uses, so I will test this more thoroughly next time (maybe I should start a test list).
On a side note, I would not completely disregard the insulin effects of fat. I say this simply noting that while they are small, they are not zero either. Have you watched https://www.dietdoctor.com/diet-doctor-podcast-24-robb-wolf . I think he makes some interesting points.
PaulL
(You've tried everything else; why not try bacon?)
#40
Insulin is necessary for life, which is why Type I diabetics die without it. But we don’t need much of a response, and we have to eat something. If you don’t want to eat fat because of its effect on insulin secretion, then you certainly don’t want to eat protein or carbohydrate, because their effect on insulin is so much greater. Protein is essential to the diet, and so are certain fatty acids. Given that fact, it hardly seems that there is any point in worrying about a potential insulin effect from food essential for life.
Bikman’s point is that in the absence of dietary carbohydrate (or when dietary carbohydrate is minimal), the insulin/glucagon ratio remains low, and the body is in a primarily catabolic state. In the normal course of things, insulin is supposed to rise while we eat, so as to cause some energy storage in the adipose tissue, then fall while we fast, so as to allow some of that stored energy to fuel the body. We don’t want a complete absence of insulin response, any more than we want the elevated insulin required to drive excessive glucose out of the bloodstream. What we want is a gentle rise and fall, within a temperate range.
Insulin resistance resulting from years of a high-carbohydrate diet takes time to resolve, but a ketogenic diet can allow the metabolism to recover to the point where we can say that a person is no longer a Type II diabetic (see the data presented by Dr. Sarah Hallberg of Virta Health). The late Dr. Joseph Kraft argued that people should be diagnosed with Type II a decade or two earlier than they usually are, and he had test data from many patients, followed over decades, to support his point. Unfortunately, the usual diagnostic for Type II is based on loss of glucose control, ignoring the struggle of insulin to contain glucose until the struggle is lost. Dr. Kraft called it diabetes in situ, or “occult diabetes.” If he was right, as it would appear, then the standard thinking about what diabetes actually is needs some serious revision.
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#41
This makes a lot of sense in the evolutionary perspectiive. If we’re going to require some small amount of glucose it’s far better to have an onboard mechanism to generate it rather than depend on eating it in an environment where edible glucose was scarce. At the same time, it was advantageous to have an antagonist that stored it when it was available.
Naghite
(Michael)
#42
woah, I never said I was worried about eating fat due to insulin response! I was just saying that you tend to disregard entirely, whereas I am implying that may be a bit too simplistic. Re: Bikman and that video. I do remember now that he ended the video https://www.youtube.com/watch?v=z3fO5aTD6JU at minute 30ish noting that people who on keto have higher I/G ratios due to metabolic issues (like T2D) might want to consider limiting protein until they resolve some of the insulin resistance, because they may have a greater effect due to starting at such an elevated ratio, whereas metabolic healthy people on Low carb are probably fine eating as much protein as desired (very end iirc as a conclusion)
PaulL
(You've tried everything else; why not try bacon?)
#43
No worries; I was just taking your comment to the logical extreme. Since fat has the very least insulin response of all foods, and it’s just the minimum required to sustain life, it tickled my sense of humour that you made a point of mentioning it.
The point of Prof. Bikman’s that you mention is well-taken, since protein does have a significant insulin response, unlike fat. And since he makes such a point of the glucagon response in a low-carb milieu, I guess if he has a concern, we should pay attention.
BuckRimfire
(BuckRimfire)
#44
I found what might be the answer we’re looking for in The Complete Book of Ketones by Mary T. Newport MD. From p. 144:
During starvation, about 80 grams of glucose is produced daily by the internal organs, of which about 10-11 grams come from ketones, 35-40 grams from recycled lactate and pyruvate, 20 grams from the glycerol backbone of fatty acids, and the remaining 15-20 grams from amino acids, mainly alanine but also glutamine.
Her references are Owen, Cahill, et al 1967 and 2005
fitbod
#45
Below is a post from Amber circa 2013 where she thought exercise was helping her get more ketones without protein restriction. I’m finding that cardio exercise is helping me manage my high-ish fasting glucose and maybe on the margin can contribute to higher ketones. All else equal, if my morning blood sugar is like 115 my ketones will be low. My cardio is a mix of low intensity steady-state with some “sprints” - i do this on an indoor bike. Theoretically at least is should be the sprints that burn more glucose.
What i think i’m pretty sure of (although it can be hard to be sure of much!) is that my morning ketones have dropped since I have become more weight stable. But I can get them up simply by drinking coffee with HWC. If I want to be extra fancy I can have some MCT oil. But I naturally tend toward OMAD so sometimes question if I should just drink black coffee and get the full benefit of fasting. Unfortunately the “benefits” aren’t measurable. I definitely have more energy if I just consume some fat in the morning. I’m leaning back towards a protocol of “fat fasting” until dinner.
It is hard for me to consume “enough” protein at the one meal but as someone who dabbled in bodybuilding for the past 30 years I unfortunately can never draw many conclusions about higher protein = more muscle. As a 46 year old male I suspect my testosterone levels might be more of a limiting factor in that regard than some grams/kg equation.