Yeah, I’m sure they’re not tying the tests to the individual. Why would they do do that?
Plenty of other countries to look at which took it seriously and didn’t treat it as a political war to be won. That’s instructive.

Yeah, I’m sure they’re not tying the tests to the individual. Why would they do do that?
Plenty of other countries to look at which took it seriously and didn’t treat it as a political war to be won. That’s instructive.
Yes, of course - but there’s such an incredibly wide range of policy, culture and results across the different countries. We can’t all be Sweden  (for so many reasons!).
(for so many reasons!).
Yes, I believe that it still is the point, as far as the authorities are concerned. The metric is how many cases require hospital beds, and whether we have enough beds and respirators to meet the need. The state of Connecticut is slowly lifting restrictions, and we are seeing a rise in cases as a result. We are hoping to limit the rise without having to go back into full lockdown again. More people are going to die, make no mistake, but we can’t stay locked down forever.
It’s a question of trading off different kinds of damage. Europe lost roughly a quarter of its population from the Black Death, and the while people eventually recovered from the emotional horror, the plague caused economic and social changes that have endured for centuries. The influenza epidemic of 1918 likewise had a profound economic effect, as well as an emotional one (my grandparents’ generation were all young adults in 1918, and my grandparents were still mourning their lost relatives in the 1960’s).
Assuming that’s the main goal - and I think most folks and policy makers have forgotten that by now - what are we aiming for in terms of hospital availability? To my knowledge (and I could well be wrong) the only time hospitals were actually overwhelmed were for a few weeks in NYC. Not to minimize that - it was brutal and thankfully relatively short - but if anything hospitals have been more empty than full for most of the US for most of the year.
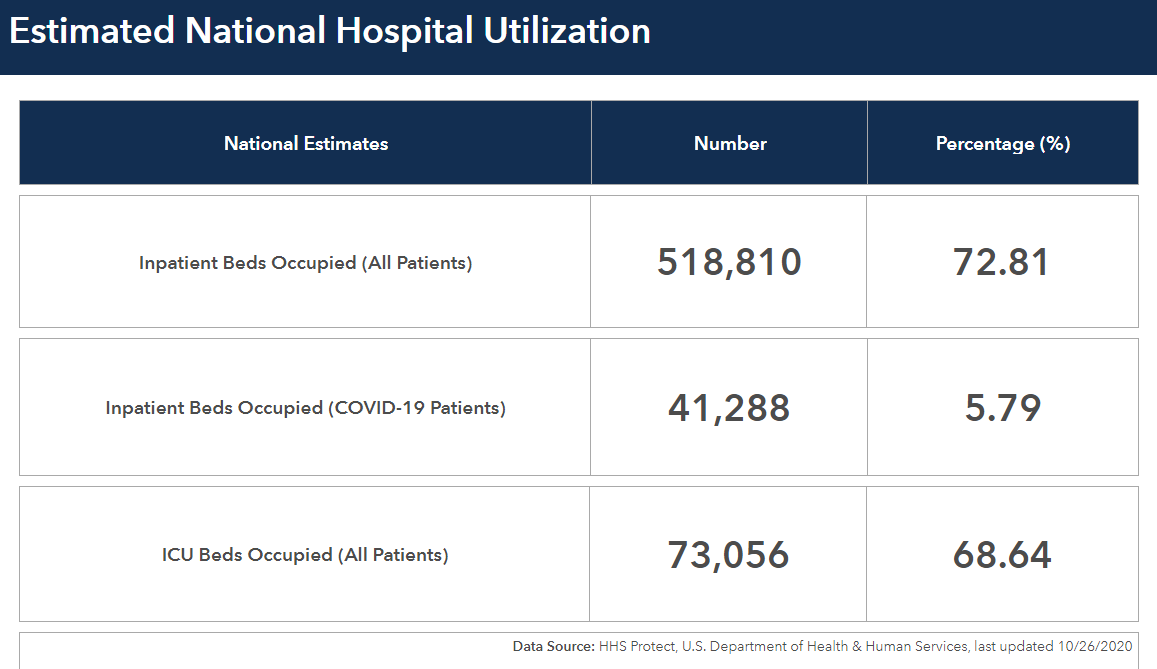
Thanks, Doug. That’s interesting. So looking at the map in your link, in CT (and most of the states that had their big wave in the spring) between 0 and 5% of the beds are currently occupied by COVID patients. In the spring, units were cleared out to make room for COVID patients and I think that other interventions tended to be delayed. By now, hospital beds are mostly full of folks with other conditions, likely with some backlog from the previous months.
Going back to @PaulL’s original point that the purpose of the shutdowns were to prevent hospital overwhelm, I’m wondering what numbers the states are looking at. Is it when the COVID cases hit a certain number in the hospitals? When we have a certain % beds available?
I can only speak about the authorities in my own state, who I know for a fact have not forgotten the reasons for the restrictions they have imposed. Whether their decisions and actions have been the best possible ones is not something I am equipped to judge, but I do know that their intentions are the best. (It’s a small state, and I am politically active.) My sister, who has a couple of degrees in public health, feels that they are doing the best they can and is comfortable both with how the state shut down and how it is now slowly opening back up. The problem with this stuff is that we can’t go back and see whether different decisions would have worked out better.
If 73% of beds being occupied is considered high (I honestly don’t know if it is or not), but fewer than 6% are covid patients, then it seems the hospitals are full for other reasons. Would 67% occupancy be alarming?
It looks like it may have been a mistake to ration other care for the past several months and lay off hospital employees. It all comes home to roost eventually.
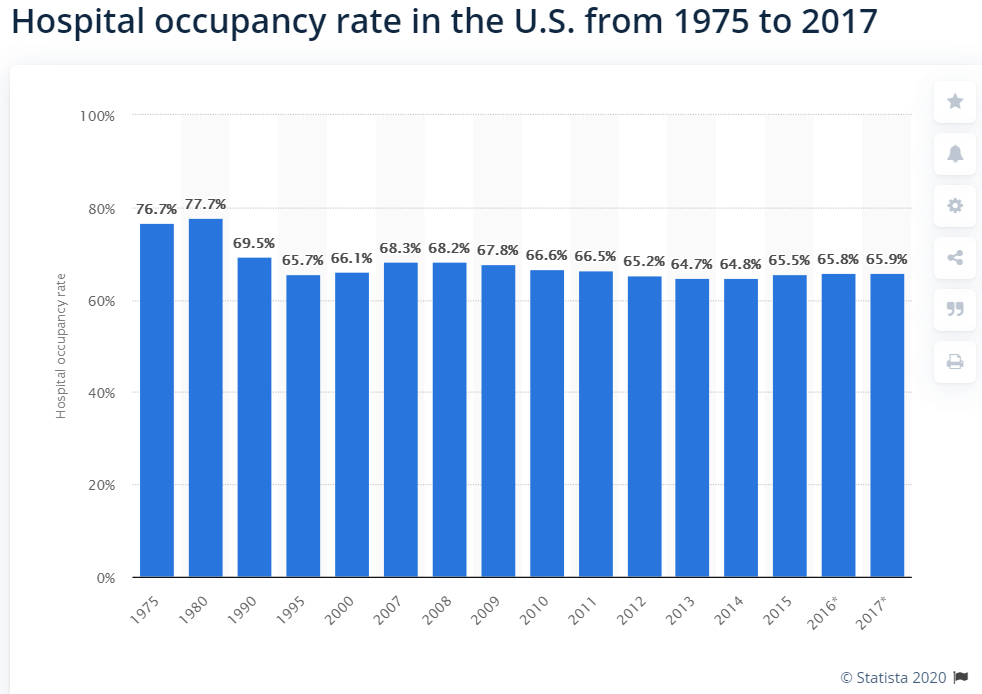
I believe around 70% is typical occupancy, but a source for that would be appreciated.
The hospitals were full of patients before COVID came along. Full hospitals are not a problem, the problem would be the nightmare of people not getting essential care for other conditions when needed, because all the beds would be full of COVID patients.
Remember that allowing this new disease to run its course unchecked would have brought personal and economic disruptions of other kinds, and if the authorities had not acted as they have, we would be complaining just as much about their lack of action as we are now complaining about they actions they have in fact taken.
There is no way to win, here; there just isn’t. Yes, we could have accepted that the hospitals, morgues, and funeral industry would have been overwhelmed for a while, while all the vulnerable people all got sick and died off, but would that have really been preferable to the restrictions that everyone finds so odious?
It’s really hard to say how things would have gone, but based on what has happened in other countries I think that less general shutdown and more targeted protection would have been much better, yes. It would have been challenging to be sure, but to have non-vulnerable folks out and about and living their lives would have given the whole society a resilience that we are now desperately lacking. In full disclosure, to my mind, part of that more targeted protection would need to include true health measures (food in nursing homes, sunlight, etc) which is probably laughably unrealistic.
I can easily believe this! Although I’m not happy with a lot of what I’ve seen in our country, I think a lot of folks have worked incredibly hard and absolutely with the best intentions.
Yes, you’re right. It’s been a series of terrible options
Yeah, Madeleine - here in Atlanta there were a couple hospitals that had essentially this condition - three normal hospital wards, including ICU, full of Covid patients. A fourth ward was opened up/cobbled together to handle other types of patients. Some patients still had to be sent to other hospitals. July and August were the busiest months thus far in Georgia - quite a bit delayed versus the Northeast.
Good question - I don’t know what the average hospital would say is an ‘overload.’ Normal occupancy is ~2/3, 66% or 67%. When NY and NJ were getting very busy with Covid patients, I remember seeing the rest of the country being in the high 50s, 60s and low 70s. The average hospital stay is significantly shorter than it used to be, but we also have far fewer hospital beds - it’s gone from 2+ million in the U.S. to 800,000 or so since the 1970s (rough guess there, from memory). Around 90,000 ICU beds, normally.
Smaller hospitals, with relatively few beds, have a tougher time keeping things where they want them. They need fairly high occupancy since they need the money coming in, but it doesn’t take too many more patients than normal before they’re stretched thin. I’m thinking that it’s not as simple as just plugging new Covid patients into open hospital beds, due to the need for isolation. If a hospital is 60 - 80% full and then has to make one hall/ward/floor just for Covid patients, it’s probably a real pain.
Darren - indeed. I wouldn’t want to be vitamin D deficient these days… Some of the low levels could be due to consumption of the vitamin - it’s definitely linked to and involved with our immune system response, so perhaps we use it up in trying to fight the virus - but either way I think it pays to be aware, here.
There have been other studies that correlate vitamin d levels to covid severity. Including one small study where some people with deficiencies were treated with vitamin d once they arrived in the hospital and had better outcomes.
And since the body synthesise vitamin D from cholesterol, that may be yet another reason not to worry about one’s cholesterol levels.
Brings to mind somebody busting their butt to lower their cholesterol while actually depriving themself of something they need. 
Doug, I’m not sure I understand this statement. Levels are low, because people are taking it, as in the vitamin isn’t as effective?
I can’t usually remember 90% of what I’ve read, but my recollection of reading about vitamin D was the best way to get it, of course is by sun exposure. If taken orally, it needs to be taken in combination with K2, and magnesium.
In one study, the data revealed a slower progression of calcification in those taking both vitamin K2 and vitamin D compared to those taking vitamin D alone.
If you take calcium and vitamin D but are deficient in vitamin K2, you could be worse off than if you were not taking those supplements at all, as demonstrated by one meta-analysis that linked calcium supplements to heart attacks.
Magnesium is also a crucial part of the equation, as it is a component necessary for the activation of vitamin D. Without sufficient amounts of it, your body cannot properly utilize the vitamin D you’re taking.
According to a scientific review published in 2018, as many as 50% of Americans taking vitamin D supplements may not get significant benefit as the vitamin D simply gets stored in its inactive form, and the reason for this is because they have insufficient magnesium levels.
That’s some of what I’ve read, anyway.
So, in summary: Vitamin D, K2, Magnesium.
I retain this information and usually forget the rest.