https://www.jacc.org/doi/10.1016/j.jacadv.2024.101049
Just came accross this. Interesting.

https://www.jacc.org/doi/10.1016/j.jacadv.2024.101049
Just came accross this. Interesting.
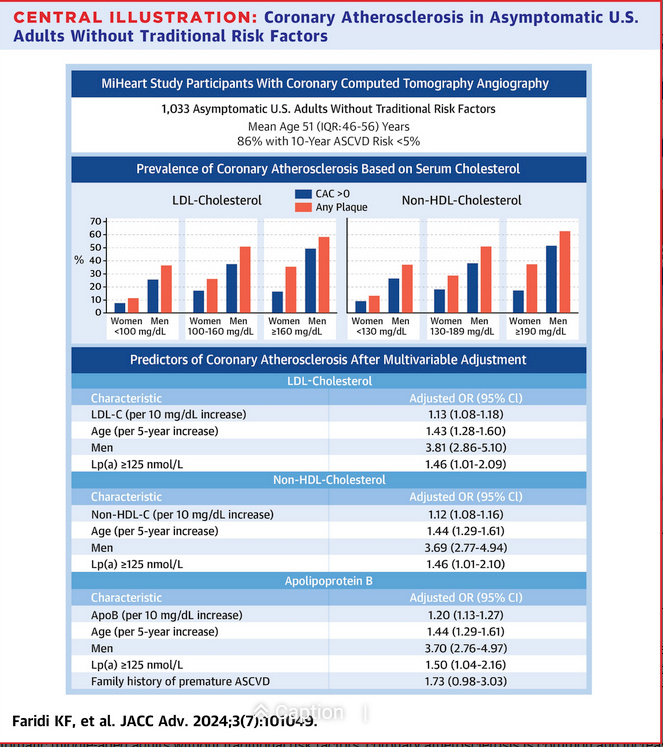
Being a male is apparently bad. Getting old is bad.
Does anyone understand how these work? What is the median against which these are used? If you have 20 points higher than that, what’s your risk if say the adjusted OR is 1.13?
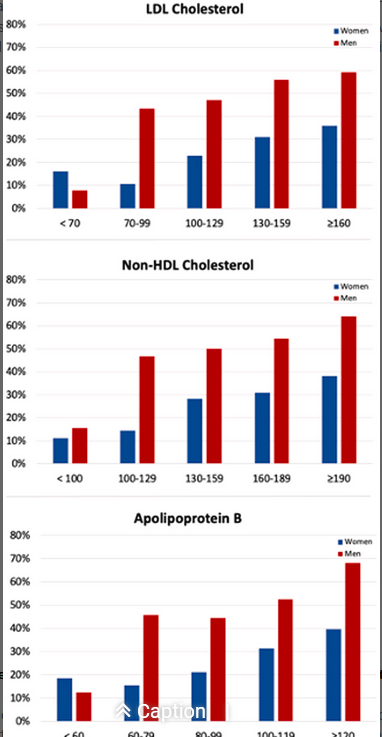
Other than the two ends, these seem to be the same to me:
Boy, I would have liked to see bar graphs with triglycerides and HDL or the ratio.
Heart disease is again the leading cause of death in the US. Yet coronary atherosclerosis, which is responsible for the majority of deaths from heart disease is easily the most preventable of the main 4 casues of death. So why does this disease remain a top killer? I believe therapies for lowering circulation LDL level-such as statins, PCSK9 inhibitors, and others have the power to virtually stop atherosclerosis.
I believe this study sheds light on the fact that CVD takes decades for it to fully present and that even those considered low risk still showed signs of cononary atherosclerosis. (“CVD risk model” is based on a 10 year window).
In conclusion, the study suggests that millions of individuals with this disease are likely unaware of it.
Me too.
@ffskier We will have to agree to disagree. If those drugs work at all, they don’t work because they lower LDL or ApoB or whatever. They work through other means.
If so, how do such beliefs square with any of these findings? …
Statins-LowCarb-Aug22.pdf (552.9 KB)
StatinAdherence-CVD.pdf (413.4 KB)
Atherosclerosis-Cholesterol-Causality.pdf (161.3 KB)
EDIT: I’ll add that the presence & level of atherosclerosis was determined by CAC Agatston scores… which only measure calcified hard plaque (believed to be the scabbing over of far more dangerous soft plaque - which is not echolucent in such a CAC evaluation).
As such, higher serum LDL-C was seen to be associated with what could be regarded as a higher level of healing the soft plaque - i.e., lower risk of future CVD, not higher.
Can one conclude that higher serum LDL-C is associated with higher incidence of CVD-related outcomes based on this study?
Absolutely! And I also believe that sticking my thermometer into ice water is a great way to deal with a fever, too!
Study 1.
“LCD to improve the most robust CVD risk factors, such as hyperglycemia, hypertension, and atherogenic dyslipidemia. Our review of the literature indicates that statin therapy for both primary and secondary prevention of CVD is not warranted for individuals on an LCD with elevated LDL-C who have achieved a low triglyceride/HDL ratio.”
But what if you have not achieved a low ratio? Or a high CAC score > 400 or a high ApoB.
“This finding supports the view that individuals on an LCD with high LDL-C and a nonatherogenic lipid profile (low TGs/high HDL-C) would not benefit from statin therapy.”
Again what if their profile was different?
Study 2 - Not sure what to make of this adherence issue.
Study 3 - Paul should keep to his magnets.
Have a look at the work of Dr. Allan Sniderman. Research cardiologist. One on the best in the world.
@ffskier Thanks for taking time to peruse the attachments. I will try to respond to each in turn…
If you’re unhealthy (e.g., ratio: high Trig/low HDL, or have evidence of massive arterial damage requiring extensive calcification to heal) then you will likely die younger.
That’s the association - perhaps like firetrucks arriving at the fire. Blaming elevated LDL-C for this situation as the cause of disease has become a contention that many researchers now dispute.
I found the summarized takeaway in #2 to be clear enough:
“Our perspective of the literature is that non-adherence to statin treatment for primary prevention of CVD is justified because the meager benefits are more than offset by the extensive harms.”
I’ll leave @PaulL’s personal magnetism for another thread  … but here are the key conclusions of Study 3:
… but here are the key conclusions of Study 3:
Cholesterol does not predict degree of atherosclerosis at autopsy.
Cholesterol does not correlate with degree of coronary calcification.
Cholesterol does not correlate with degree of peripheral atherosclerosis.
Cholesterol does not correlate with degree of coronary atherosclerosis on angiography.
Am sharing these studies not to be argumentative, but to simply point out that there is considerable reliable evidence that taking statins to lower LDL (along with other lipid components that decline with it) is not a good way to improve health, reduce mortality, nor reduce risk of CVD attributable to atherosclerosis.