
Does anyone have any experience with the above statin alternatives?
PCSK9 Inhibitors, Ezetimibe and Bempedoic Acid as Statin Alternatives?
Alecmcq
(Alec)
#2
Yes. I was told by my doctor that I needed to be on a PCSK9 inhibitor to “treat” my 450 level LDL “problem”. I told him he could file his PCSK9s in the same place I invited him to file his statins.
I struggle to understand why doctors want me to die earlier by reducing my LDL level. Makes no sense. Or maybe they just think I am too much of a PITA.
ctviggen
(Bob M)
#3
450? Have you reached LMHR status?
PCSK9i haven’t shown great results, if I’m remembering correctly.
ffskier
#4
Is that 450 mg/dL ? if so this puts you in the HoFH range. Very rare, like 1 in a million This means you inherited the genetic variants from both parents not just one.
Alecmcq
(Alec)
#5
Yes, mg/dl. Do I have FH? Possibly…. All my siblings also have crazy high cholesterol. My parents died of unrelated diseases aged 82 and 86. They never had their lipids tested. Crucially, my current CT scan score is 10… ie not zero calcification, but still very low.
Is it 1 in a million, I don’t think so… It might be quite rare, but I hear of this kind of level in the carnivore community quite often. Admittedly, that’s a very small community…
I have some features of LMHRs but not all. I am “leaning” but not lean  . My trigs are higher than LMHR standard, also my HDL is slightly lower than LMHR standard. But do I believe that some of the processes going on with LMHR are going on in me? Yes, yes I do…
. My trigs are higher than LMHR standard, also my HDL is slightly lower than LMHR standard. But do I believe that some of the processes going on with LMHR are going on in me? Yes, yes I do…
Am I in any way concerned about having that level of LDL? Nope. Very happy, as from the research I have done “high” LDL is protective against all cause mortality. I’m happy with that!
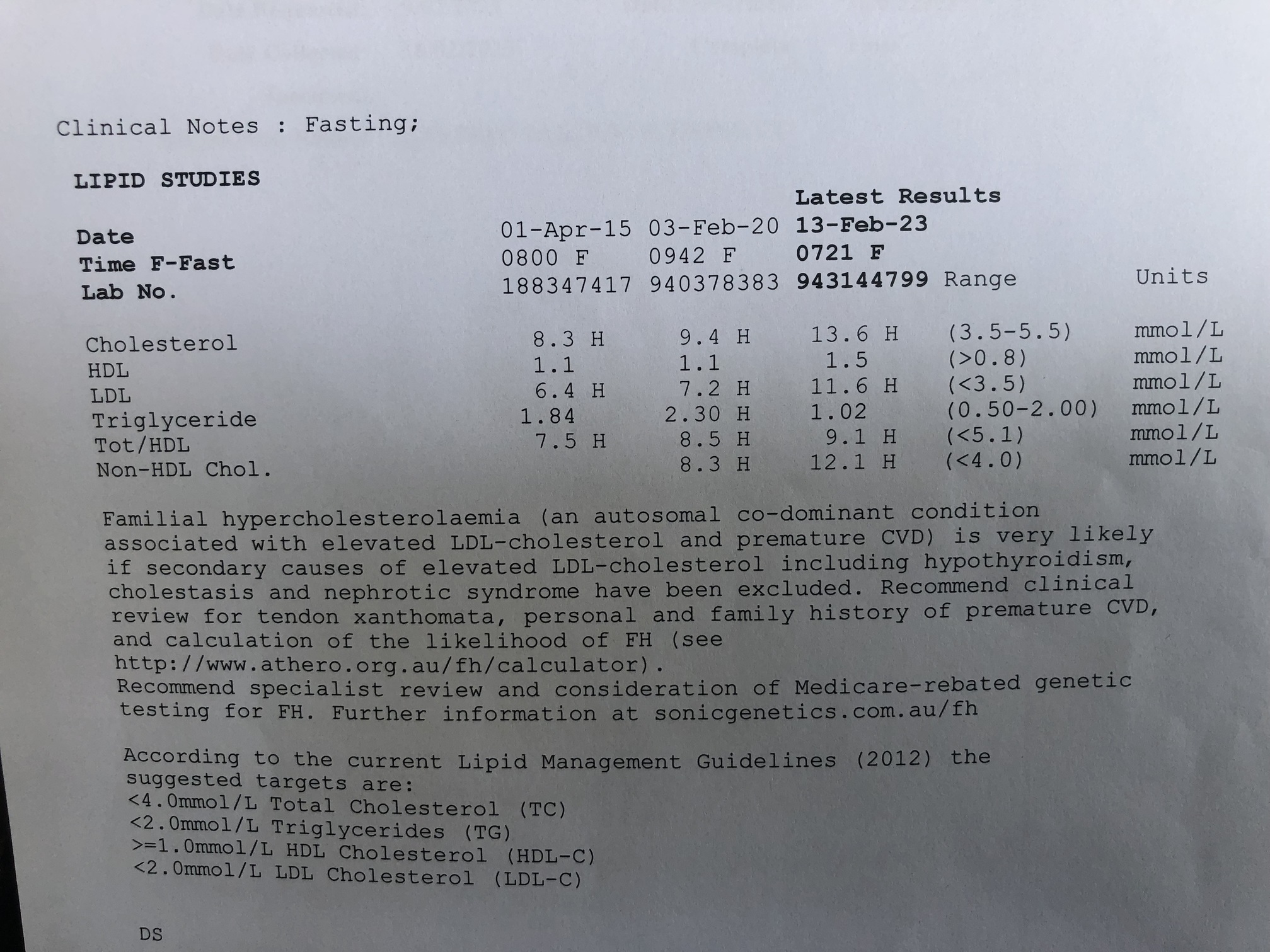
In case anyone is doubting this crazy high LDL level, below is my latest report… it’s in mmol/L, but 11.6mmol/L = 450mg/dl. You’ll note that the report does mention FH. I love that the high end target is 2.0 and I am 11.6. You can see why my doctor crapped himself The Medical Establishment think I should be dead by now. I just get on with running half marathons.
ctviggen
(Bob M)
#6
I’ve seen people with higher LDL. Dr. Unwin’s wife, Jen Unwin, who wrote this book:
Has some insanely high LDL, but got either a CAC scan or a better scan done, no indication of atherosclerosis.
Alec, your trigs are coming down and HDL is going up, so that’s good.
The “problem” with LDL is (like pretty much everything else) that it’s multi-faceted. People think it just clogs arteries, but it operates to shuttle energy around (one reason LMHRs get higher LDL) and acts as part of the immune system.
If you do have FH, then one concern could be coagulation. There’s a theory people with FH have errors in coagulation. I’m not sure how to address that, though. Certainly keto helps, as it’s less inflammatory. Something like CRP or sedimentation rate might help see what the risk is. But then if those are higher (my CRP is generally under 1, but supposedly it’s supposed to be under 0.3 – not sure what units), I don’t know what to do to get them lower. I have extremely high Lp(a) which also might have coagulation issues. Just don’t know how to address those.
robintemplin
(Robin)
#7
This reminds me of the first cardiologist I fired. He walked into the room, said my LDL was the 2nd highest he had ever seen and would be putting me on the latest injections $$$$$. No discussion, no questions.
To answer the original poster, I now take simvastatin and ezetimibe and warfarin. Yes, I have sold out…. And swimming against the current here.
But after several strokes, memory loss, and ongoing AFib (all while carnivore) I’m just covering all my bases. Carnivore, exercise, and drugs. (different doc tho)
ctviggen
(Bob M)
#10
You might have some type of coagulation issue. It might not be your LDL per se. See this for instance:
https://www.sciencedirect.com/science/article/abs/pii/S0306987718304729?via%3Dihub
Hmm…I thought I had the full study somewhere, but this seems to be behind a paywall.
They say that one drug has some benefit, due to its anti-coagulate effects: probucol.
The problem is that everyone has been focused on LDL for so long that no one has thought about anything else. How do you address errors in coagulation? I don’t know.
I assume reducing inflammation would help, and keto/carnivore should help there. I assume blood thinners (as you’re on) might help. But there might be something better, but since everyone thinks all you have to do is reduce LDL and everything is good, that’s all you get. It’s the whole “when all you have is a hammer, all you see is nails” idea.
robintemplin
(Robin)
#11
@ctviggen Yeah…. The hammer and nail is a very real thing. I’m fortunate that my GP and cardiologist (new) both support keto and carnivore and acknowledge its benefits for heart health.
I definitely had coagulation issues… but seem to have landed in a good place for now. No one really talks about my ldl these days. I do have the option of dropping the statin, and I understand the risks of taking one.
But I feel great. Mental clarity and high energy have returned.
So for now…. I am calling it good enough.
lfod14
#12
Statins vs PSSK9 is really a specific to you thing, if your body is making too much, Statins are better, if your body isn’t really making too much, but you can’t clear it, PCSK9 is the correct one. The sides are similar in both, so really semantics at that point. They’re both blocking enzymes to lower cholesterol, just different ones that use different pathways.
Real question is can you really not lower it on your own, do you track what you eat so you have an idea of what’s coming in? Many people simply can’t take in the amounts of fat that is normal on keto, and simply lowering it does the trick. But if you’re not tracking you have nothing to go in. I’m one of them.
On alternatives, Red Yeast rice (only if it’s real) will help it decently. Ezetimibe and BA as far as I know are usually last resorts because of lowered efficacy.
Alecmcq
(Alec)
#13
I wasn’t at all disappointed with these levels… they are just away from the defined LMHR levels. Re coagulation… yes, I have been aware of that risk, but my blood does not seem to be sticky in any way.
I have wanted to get a CAC scan for a long time, and it has proved difficult. When you have “very high” LDL levels, there is always the CW bell ringing in your head (what if I am wrong?), so I have been looking for a way to get a CAC scan done. I went to the Dr about a year ago and asked for a metabolic health check to just see where I was. In that I asked for a CAC scan… dr said no. But when those results came back, doctor went deep end, and agreed to get me a scan, but said it had to be a CT scan (which he said would pick up soft plaque as well as the calcium). Result was 10, which is not zero but very low, and both the Dr, the report, and the specialist interpreter of scan said I was at “very low risk” of CVD with that scan.
I am 60. Most of my life I have eaten crap. So I have been lucky (so far), but I have had high to very high to stratospheric LDL all my life… and yet I have a CT scan score at age 60 of 10… this is my primary evidence that I personally have that for me “high” LDL has not caused CVD. I also believe the other evidence that there is that LDL is not causative in CVD. So, my view is there is NO reason to reduce a natural level of LDL.
robintemplin
(Robin)
#14
I was strict keto for one year. Strict Carnivore for 2 years.
I tracked religiously. My food intake is one thing I am 100% on top of. As an ex-addict…. I draw a hard line in the sand and DO NOT CROSS.
PaulL
(You've tried everything else; why not try bacon?)
#15
About 50% of them do, and those are the ones that develop cardiovascular disease. The ones who don’t have the coagulation mutations are the ones who live long lives and die of unrelated causes. This has been known since the 1960’s.

ffskier
#18
No, you did not sell out. You took reasonable actions based on your own experiences. That is being called responsible. If interested, take a look at some of the studies done on the Norwegian population. They have a higher level of FH on a per capita basis than most places.
I wish you the best of health.
robintemplin
(Robin)
#19
Thanks @ffskier. I don’t believe I sold out either, but I do at times feel guilty admitting my medications on this forum.
ffskier
#20
Think of it another way. You had the courage to admit something that the vast majority of people would never do on a public forum. You are not responsible for their care, and neither are they responsible for your care. Also, keep in mind that many people distrust authority, except when it confirms their narrative. I previously mentioned looking up studies on Norway and FH. You may also find Dr. Allan Sniderman of some interest.
Google: #185 – Allan Sniderman, M.D.: Cardiovascular disease and why we should change the way we assess risk