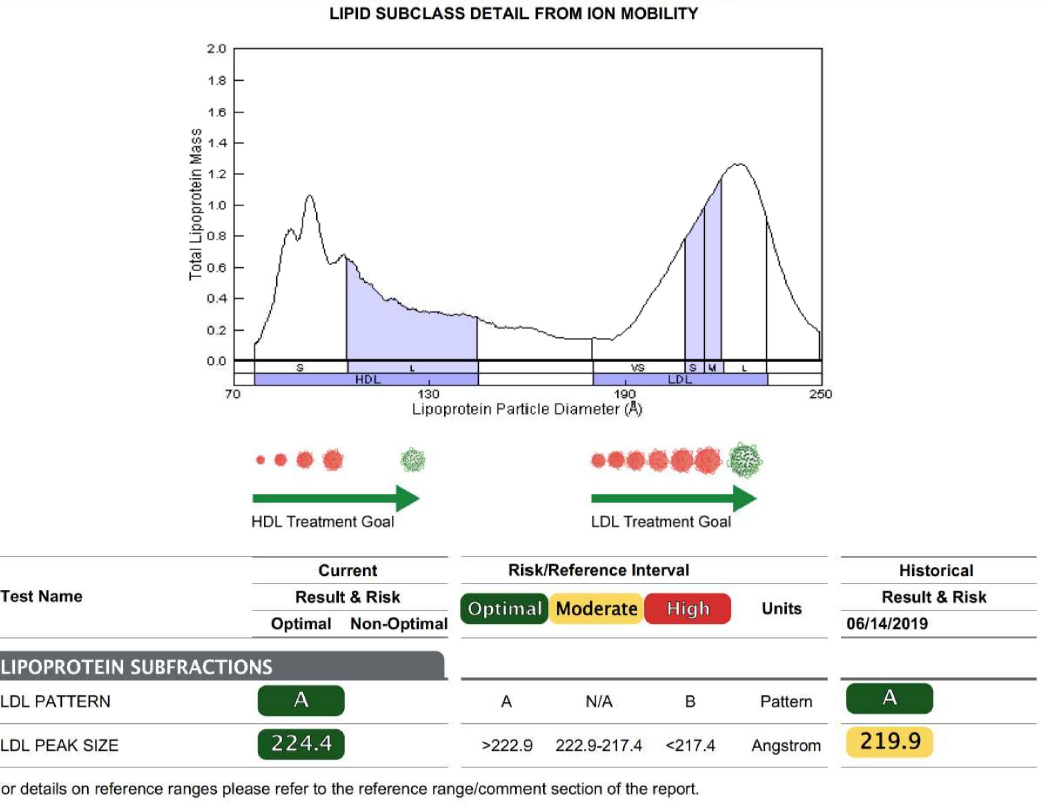
With a triglyceride/HDL ratio of 1.0, you are fine. If your physician had ordered an NMR test of your LDL, she would have discovered that it is all the healthy, low-risk Pattern A, and therefore not a problem. The CAC scan will provide a far more accurate estimate of your cardiovascular risk. Your challenge to her echoes Dave Feldman’s. I’d be interested to hear her response.
In the days before statins were developed, an LDL level of 172 was considered perfectly healthy. The manufacturers have steadily lowered the “healthy” level in order to create more market for their product.
Some facts you can give your physician to try and urge her to think:
-
Well over half the people who arrive at the emergency room with their first heart attack have normal, or even low, LDL levels. Is this what we would expect if LDL causes heart disease?
-
Of the people with familial hypercholesterolaemia, about half never have a heart attack, never develop cardiovascular disease, and die at perfectly normal ages of other causes. By some weird chance, the half who do have heart attacks and die young, all just happen to have genetic abnormalities (mostly variations in their fibrinogen or their clotting factor VIII) that cause their blood to clot more readily. This has been known since the 1960’s.
-
Several large, government funded studies have demonstrated, not an association between high LDL or total cholesterol and higher rates of cardiovascular disease, but rather an inverse correlation between low cholesterol and higher disease rates and mortality. In fact, the correlation between higher cholesterol and lower rates of mortality and CVD seems to get stronger as we age. Among these studies are the Nurses Health Initiative, MRFIT, the Framingham study, and Ancel Keys’s own Minnesota Coronary Study (which went unpublished for 17 years, because it failed to demonstrate any connexion between cholesterol and coronary heart disease).
-
Not only is cholesterol an essential component of the wall of every cell in our body, it is a major component of brain cells and is essential to proper functioning of our neurons. Not only that, but it is a precursor to a number of different chemicals in the body, among them vitamin D and the sex hormones progesterone and testosterone. Cholesterol also plays a vital role in the immune system, helping destroy invading bacteria.
-
(This is my favourite:) While cholesterol is indeed present in atherosclerotic plaque, it now appears to be there as part of the body’s repair mechanisms, and not as the cause. This makes blaming cardiovascular disease on cholesterol very much like blaming fires on fire trucks. (They’re present at every fire, right?)
Hope this helps you persuade your physician to see reason. You might also mention that there is a group of physicians and researchers, called the International Network of Cholesterol Sceptics (THINCS). Their Web site contains some very interesting data, from which they draw some very interesting conclusions.