
Hey guys,
TL;DR: I’m a 37 year old Aussie living in NY who’s super happy on keto. I’m eating delicious food, get satiated quickly, and I’m slowly losing my last few pounds. But: I am planning to try switching out some of my saturates for monounsaturated fats as I consider what this lifestyle will look like for me in the long term. Heresy!
So I was waiting until most of my latest results came back to do this post, and now I’ve got them. I’ve been on LCHF since July 2016, and keto for 2-3 months now. I was 93.5kg at the start, and quickly dropped to 83.5kg within 3 months. I plateaued for 9 months or so, and since going keto I’ve dropped another 3-4kg in the last couple of months.
About a month ago, I got blood test results back for the first time in a while: HbA1c of 4.8 (though this wasn’t unexpected, I’ve happily had no sign of IR before, even though I’m convinced I was probably on the way), fasting glucose 87, great liver (AST/ALT) results (I’d had fatty liver seen via ultrasound before and elevated liver enzyme results), and the following lipid panel:
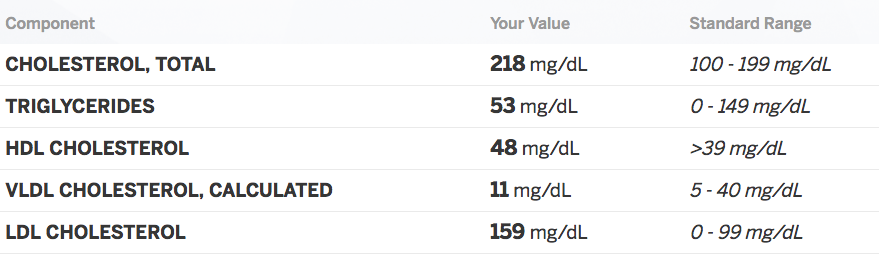
As you can see, elevated cholesterol, great trigs, meh HDL, good VLDL, but borderline high LDL that had TRIPLED since October of last year. That worried me, and I am totally unconvinced by the ketoers who claim that LDL is irrelevant.
I wanted an advanced lipid panel. My GP here in NYC wouldn’t give me one, and referred me to a cardiologist. I thought this was overkill, but 2 weeks later when my appointment came, I was happy I’d have a chance to challenge him and discuss the keto lifestyle with him.
I spent an hour with the cardiologist. Lovely guy, not opposed to low carb, but rather insistent that there’s plenty of science to show that meat products/sat fat elevate CVD risk, and insufficient evidence to show that LCHF diets are safe in the long term when it comes to CVD.
I thought I’d have to talk him into doing a calcium score, but he was very keen to have me do it. I’ve scheduled it for 2 weeks from now. In the meantime, we did C-reactive protein and an advanced lipid panel (NMR).
CRP came back 0.99, which is nice and low. It had been 2.2 last October after just a few months on LCHF.
Here are my NMR results:
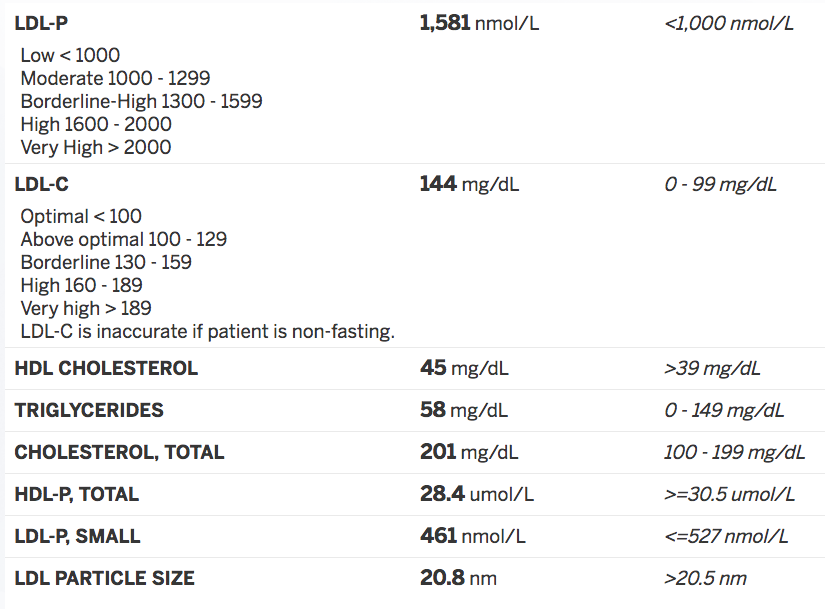
I don’t need to tell you that these results are mixed. On the one hand, my small dense LDL are relatively low, but I don’t fit neatly into Pattern A or Pattern B when it comes to the distribution of particle sizes. HDL not brilliant still. And to add to the confusion, the cardiologist noted that there’s not much data on NMR results anyway, so it’s hard to tell much from the test anyway.
We fully expect my calcium score to come back a zero. I haven’t been low carb long enough for it to affect my arteries really one way or the other.
I’ll see my cardiologist in a couple of weeks after the calcium score comes back. In the meantime, we had a chat just before the weekend, and he was perfectly amenable to me continuing LCHF for some years. I’m relatively young and as long as the calcium score comes back ok, I’m low risk and so he sees no need to be overly cautious in a conventional sense. I’m happy on keto, so he’s happy to see me continue on it.
However: it is becoming increasingly clear to me that one of the likely causes of my LDL tripling – and perhaps of my less than stellar overall cholesterol and HDL results – may be saturated fats. Specifically red meat consumption, lots of butter and cream.
I know. This is heresy. Then again, Peter Attia has made exactly this point: that SFA consumption may not be uniformly safe across the entire population.
So here we are: I’m very happy, most of the markers are good, but I am rather unconvinced by the ketoers who deny LDL is an issue and who maintain that you can eat as much SFA as you like without consequence. Show me the science. I am a healthy 37 year old man who should not be seeing his LDL triple within a year.
We are not anti-science. I got into this because I was convinced by the science. We are not conspiracy theorists who believe the entire medical establishment is brainwashed. I have a very intelligent, open-minded cardiologist (not to mention another exceptionally well-regarded genius in the medical profession with whom I’m in touch) telling me my cholesterol is something to be concerned about, and is something that might be addressed by switching out some meat and dairy for more fish and monounsaturates.
Now again, I am not opposed to running the experiment for longer, and I’ll be talking to the cardiologist about the benefits and dangers of simply continuing eating creamy sauces and loads of beef fat for another year or more. But I think that in order to continue this lifestyle in the long term, I need to consider now the balance of fats and whether keto (as opposed to simply low carb non-ketogenic) is more suitable for me as a lifestyle.
Would be fascinated to hear your thoughts.
P.S. Interestingly, of his own volition, the cardiologist brought up intermittent fasting (IF) as another thing I should consider doing. Amazing!
