
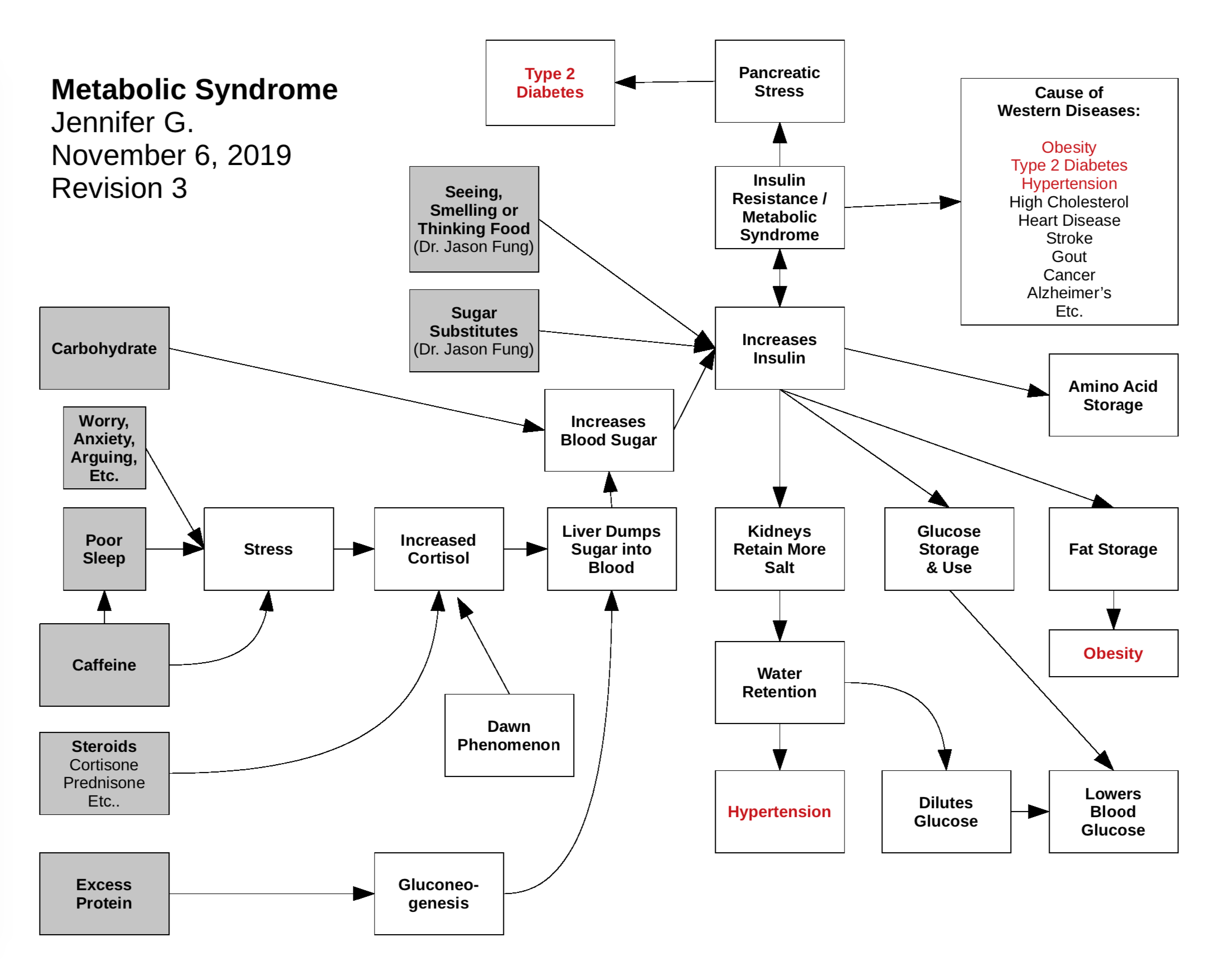
Just to visually summarize what I’ve learned so far from various Taubes, Phiney/Volek, Moore, Fung, etc. books. I just started it so I need to expand it more (e.g. how fat is created from excess glucose, pathways to the other diseases I listed, etc… Just thought I’d share. I don’t recall seeing any diagram like this before anywhere, I kind of searched for it before I drew it up one morning recently. I just wanted something simple to look at to remind me of how everything works together.
Metabolic Syndrome Diagram I've Been Working On
OgreZed
#2
Gluconeogenesis can convert either proteins or fats into glucose. But it’s based on the demand for glucose, not on an excessive supply of those proteins and fats. Otherwise, in my pre-keto days when I was eating far more proteins and fats, my arteries would have been pure glucose. 
For someone on keto, the vast majority of glucose is their body will be coming from GNG, simply because there aren’t many carbs coming in.
One question I’ve asked – what is a “low” or “normal” range for BG levels when someone is in ketosis? Glucose is no longer the source of energy for most of the body, so the “old” levels shouldn’t apply. I’ve seen anecdotal discussions where people are claiming they have BG levels in the 30’s and 40’s without the normal “low BG” symptoms – dizziness, sweats, shaking, etc. They say they feel fine.
KetoCancerMom
(Cancer Fighting Ketovore :))
#3
When I’m fasting I can get my BG into the low 50’s and maybe 40s, but not normally. Normally I’ll run in the 70s to 80s, with some upticks to the 90s.
ctviggen
(Bob M)
#4
I think to get that low, they’d have to be fasting for multiple days.
@Jennifer72 The main thing I see missing, and I don’t think it can fit, is number of meals per day.
ctviggen
(Bob M)
#5
I run on average 20 points higher. My blood sugar starts near 100 in the morning, then will go down into the 80s or even 70s. But if I exercise a lot, I can easily keep a blood sugar above 100 the whole day.
atomicspacebunny
(Bunny)
#7
More info for your diagram:
[1] Here’s What Actually Happens in Your Body When You Eat Fat
[2] The body’s own fat-metabolism protects against the harmful effects of sugar
Ketones (acetoacetate) help protect you from the glycating effect of methyglyoxal rather than a strictly glycolysis metabolism.
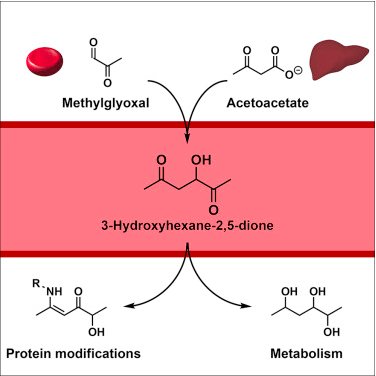
image link[3] ”…“Red meat and resistant starch have opposite effects on the colorectal cancer-promoting miRNAs, the miR-17-92 cluster,” said Karen J. Humphreys, PhD, a research associate at the Flinders Center for Innovation in Cancer at Flinders University in Adelaide, Australia. “This finding supports consumption of resistant starch as a means of reducing the risk associated with a high red meat diet.” …” …More
[4] “…MicroRNAs (miRNAs) encoded by the miR-17-92 cluster and its paralogs are known to act as oncogenes. Expression of these miRNAs promotes cell proliferation, suppresses apoptosis of cancer cells, and induces tumor angiogenesis. …” …More
[5] “…a lot of the microbiome bacteria that are fermenting a variety of fermentable fibres start to leave and you actually start to get bacteria cropping up that ferment amino acids.” These amino acid fermenting bacteria are known as putrefactive bacteria. Two products of putrefactive bacteria, putrescine and cadaverine, are best known for literally smelling like death. They are also genotoxins known to damage the DNA inside your colon cells. …” …More
[7] The accumulation of intramyo/hepatic cellular lipids/triglycerides (pre-oxidation of dietary carbohydrates vs. post-oxidation of adipose lipid droplets or ketogenic diet)
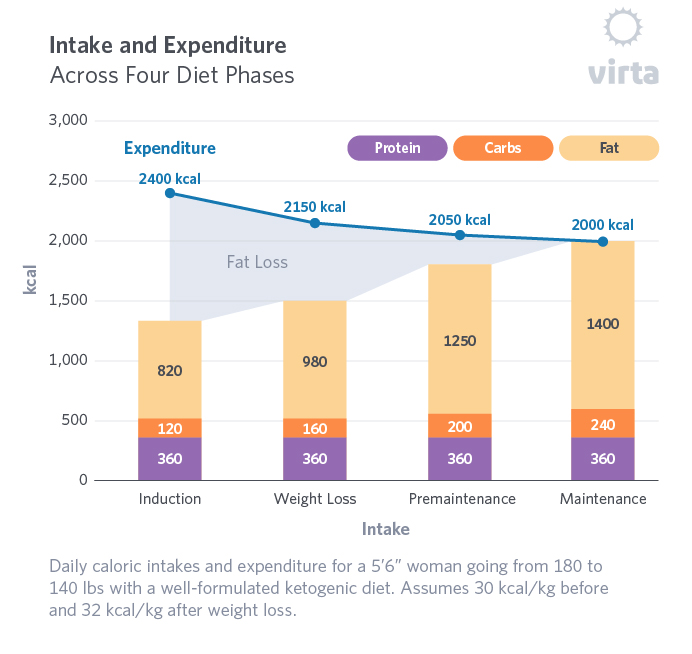
[8]
This graph illustrates a typical physiological weight loss response to a well-formulated ketogenic diet eaten to satiety rather than when prescribed as a rigid caloric restriction. Note that in this scenario, dietary protein is moderate and unchanged, carbohydrate is held constant or only slightly increased in a narrow range, and one’s spontaneous intake of fat increases to sustain satiety as major weight loss transitions into weight maintenance. …More
[10] TOFI (thin-outside-fat-inside): is used to describe lean individuals with a disproportionate amount of fat (adipose tissue) stored in their abdomen. …More (High Fructose Corn Syrup HFCS in large amounts is turned directly into visceral fat by the liver)
SlowBurnMary
#8
That’s great! I don’t know how you can fit it in - but you could add Dr. Eades’ point about carbs-first eating incretins raise insulin, whereas protein-first eating’s incretins do not.
Jennifer72
#9
Wow Mary, I’ve never heard of that before. Guess I have some more learning to do! Do you recommend a particular book I read? Is it in Protein Power… it’s a book I’ve been meaning to eventually read.
SlowBurnMary
#10
I think it’s vaguely pointed to in PP, but it wasn’t proven out yet. It’s quite compelling how glucose can stay low, but insulin surges can be high when the upper GI tract is faced with carbs before protein. Dr. Michael Eades is great - and his presentation at Low Carb Denver 2019 covers the current science on it and his synthesis of what it means when combined with LCHF/keto. I need to re-watch it to memorize certain things still, but yes, there are names for the two types of incretins, and that could be handy for your chart!
(Other interesting stuff for your chart would be Dr. Anna Cabeca’s work on lowering insulin & cortisol through boosting oxytocin, alkalinization, and practicing IF - but that would take up more space!)

Jennifer72
#11
SlowBurnMary, I want to really thank you for sharing this video with me. It’s been an eye opener! I’ve done low carb and keto for years now and really knew nothing about incretins, and especially the effect of fat mixed in with carbs. Fat alone doesn’t raise insulin much. Carbs alone do. But if you take the carbs + the fat it like skyrockets the insulin… so interesting… Thanks again!
I think from now on I am going to eat my berries, whole and alone. I have been mashing them up and mixing with lots of heavy cream and stevia for an ice cream like treat most days. Now I know why I craved that, because it could raise insulin levels higher than if I ate them separately. I am really doing all I can, in ever way, to reduce insulin. I want to reverse my severe insulin resistance (current HOMA-IR of 3.61).
I’ve shared this videos with friends and they really enjoy it as well. Dr. Eades is so awesome… I haven’t read his Protein Power book but I need to, and then buy his Protein Power 2.0 book he’s going to be coming out with soon. (Also can’t wait for Gary Taubes new book The Case for Keto.)
Jennifer72
#12
SlowBurnMary, so how does the revised chart look? Please let me know if I need to clarify what you/Dr. Eades are saying any better:
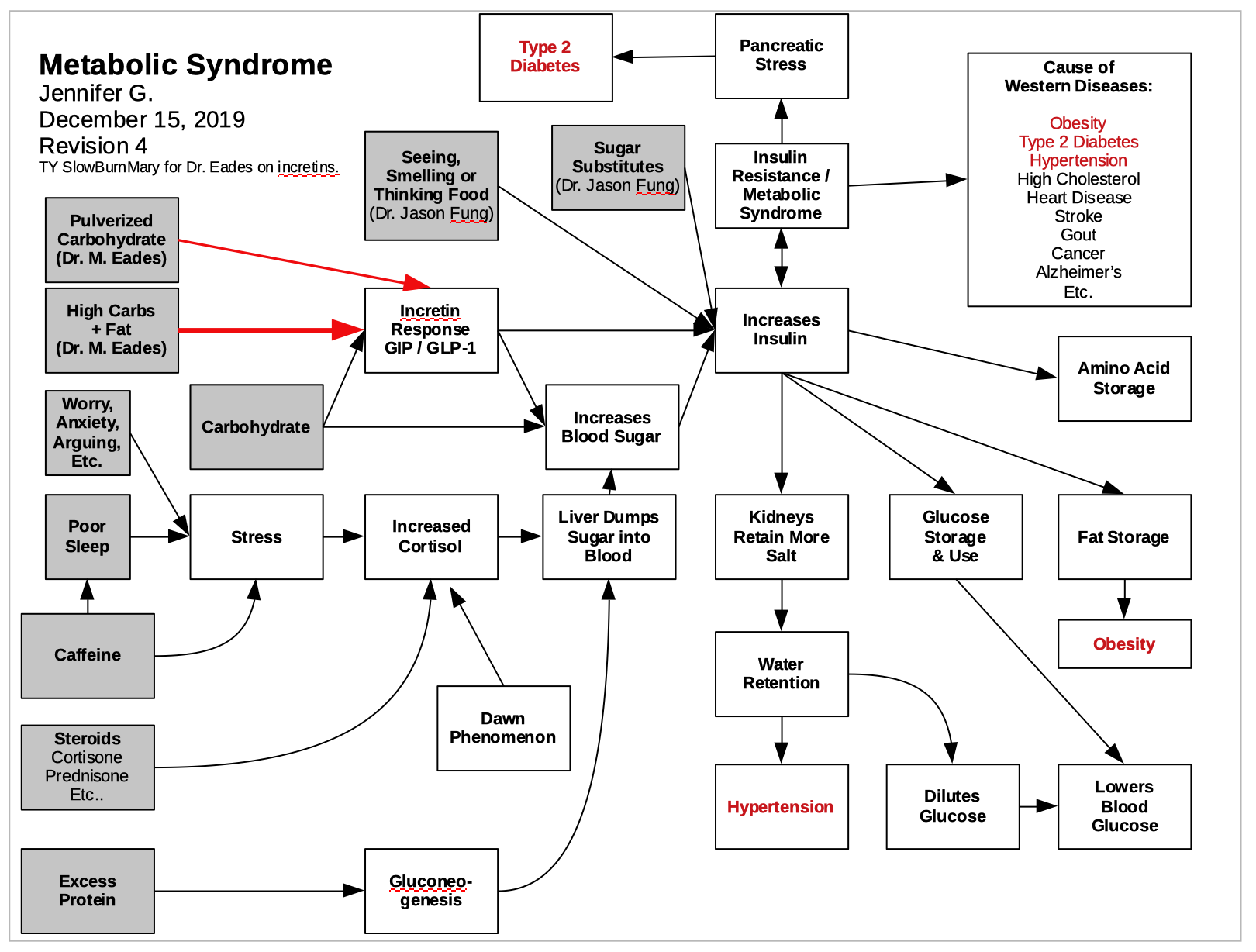
Okay I see I left out eating frequency and eating order… I’ll have to work those in later. I am gonna have to make this chart 11 x 17 i think instead of 8.5 x 11
Jennifer72
#13
By the way, the info is amazing what you provided thanks! I’ll have to read it carefully and study it all. It’s quite a bit for my pea sized brain, but I’ll get there. Will definitely update my chart with info you provided thanks!
SlowBurnMary
#14
Looking good, fabulous, great!
Am not sure that the incretins that respond to carbs-first have anything to do with blood sugar response, as Dr. Eades showed the incretins only acting on insulin levels.
Also, prob would be good to use the specific incretin type indicator, as the incretins that are stimulated by protein-only are our friends, etc. But I don’t remember those acronyms, they’re in the video. 
Jennifer72
#15
Dr. Eades says glucogon is released if needed to cover the spike in insulin from incretins, so our blood glucose doesn’t get too low.
He said fat doesn’t really raise insulin much but combined with the carbs it is raised like twice as high. There is hardly any glucose in fat so since insulin is raised high, there has to be glucose released from liver to balance the insulin spike else our bg would get dangerously low.
SlowBurnMary
#16
Right - OK it’s just that the two different incretin types are very different, and wouldn’t want folks thinking all incretins are bad. The ones that respond to protein-only are allies, etc. There are two different terms for 'em, etc.
