
I’d be very surprised if your trig/HDL ratio was under 2.0/0.9 (the latter for you, no?) and your LDL turned out not to be Pattern A. That should probably be reported to Dave Feldman, to see what he could make of it. Assuming he hasn’t already encountered and addressed that type of situation.
Lipid panel!
gabe
(Gabe “No Dogma, Only Science Please!” )
#22
My trig/HDL was 1 last I checked, and I’m about to do NMR again but last time it was decidedly not Pattern A. Happy to report upcoming results to Dave.
PaulL
(You've tried everything else; why not try bacon?)
#23
I’'m sure Dave would appreciate it. Sometimes we learn more from outliers than from the people in the center of the bell curve. I’m sorry you’re faced with all these complications, Gabe. It would be really nice if you could make some more progress.
David_Stilley
(Full Metal KETO AF)
#24
Mine still says it’s bunk, but I abstain before a blood draw for triglycerides.
@aperezY2K I seem to remember seeing something recently that small particle LDL is from sugars being turned into triglycerides. Also that the reason they cause arterial plaque is because they are able to wedge under the surface of inflamed arteries and that’s why they collect and cause vascular disease (atherosclerosis here  ). Make sure you get the 14 hours fasting time in, maybe cut back to one coffee the day before and none on the morning of the draw. Eating saturated fat will raise HDL but I needed large fish oil doses to get my triglycerides back in order after cutting my dose down for three months and crossing back over the good line. I take 1600 EPA + 1200 DHA daily. I spend about $20 a month but I feel it’s worth it. If you aren’t eating grass fed/pastured/wild caught everything the omega3 content is significantly less.
). Make sure you get the 14 hours fasting time in, maybe cut back to one coffee the day before and none on the morning of the draw. Eating saturated fat will raise HDL but I needed large fish oil doses to get my triglycerides back in order after cutting my dose down for three months and crossing back over the good line. I take 1600 EPA + 1200 DHA daily. I spend about $20 a month but I feel it’s worth it. If you aren’t eating grass fed/pastured/wild caught everything the omega3 content is significantly less.

KidKeto
(Cristian Lopez)
#25
Keep in touch with me, I eat a more paleo based diet with 50 net carbs usually not counting fiber. I switched out most if not all my saturated fats for monsaturated fats and omega 3s. Suddenly my acne was gone, I didn’t feel oily all the time, and I actually started losing more body fat 12% down to 10% (It initially wasn’t my goal but athletics were definitely toned ). My cholesterol is 150 now with an 80 as hdl and half my calories coming from fat. I can’t afford grass fed meat so I think a big thing here was that I was eating additional high omega 6 meat to the nuts and seeds I still eat to this day. I thought I was a unique case but you sound similar to me, though my way of being doesn’t allow myself to eat grains or dairy. I’ve been enjoying lots and lots of veggies, winter squashes, berries, grape fruit, nuts/seeds, avacados and lean meat, & fatty fish. Feeling great! I also do intermittent fasting so usually around hour 12 of 18 I’m at 0.8-1 mmol ketones.

gabe
(Gabe “No Dogma, Only Science Please!” )
#28
OK so I didn’t want to start a new thread, so I thought I’d continue this one because I got my NMR lipoprofile back yesterday, and I thought it would be interesting to hear if anyone has any deep knowledge on this. I’ve been doing low carb for 3 years continuously, occasional cheating but my default mode 99% of the time is LCHF. I could regale you with my weekly menu, but suffice to say that today I had:
- 2 instant coffees with a bit of HWC
- 2 small sugar free jellos (cheat)
- salmon stuffed with feta and asparagus with a side of broccoli (first non-fat calories of the day, around 4pm)
- a bit too much 72% dark chocolate (CHEAT!)
- miracle noodles with tomato/onion/cream sauce and a couple of chicken thighs with skin
- 1.5 tablespoons of peanut butter
Some days have less dark choc, and some days have more, and I often IF till as late in the day as possible, but even today my blood glucose has been below 100 for most of the day and below 90 for probably the majority of it – and the last two days have been even better. I likely dip in and out of ketosis, though I haven’t checked since pee sticks went out of fashion 3 years ago.
With that throat clearing aside, my HbA1C is 4.7, CRP is 0.4, fasting BG of 87, ALT and AST in the early-mid 20s, calcium score of zero, LPA <6, and here’s my NMR:
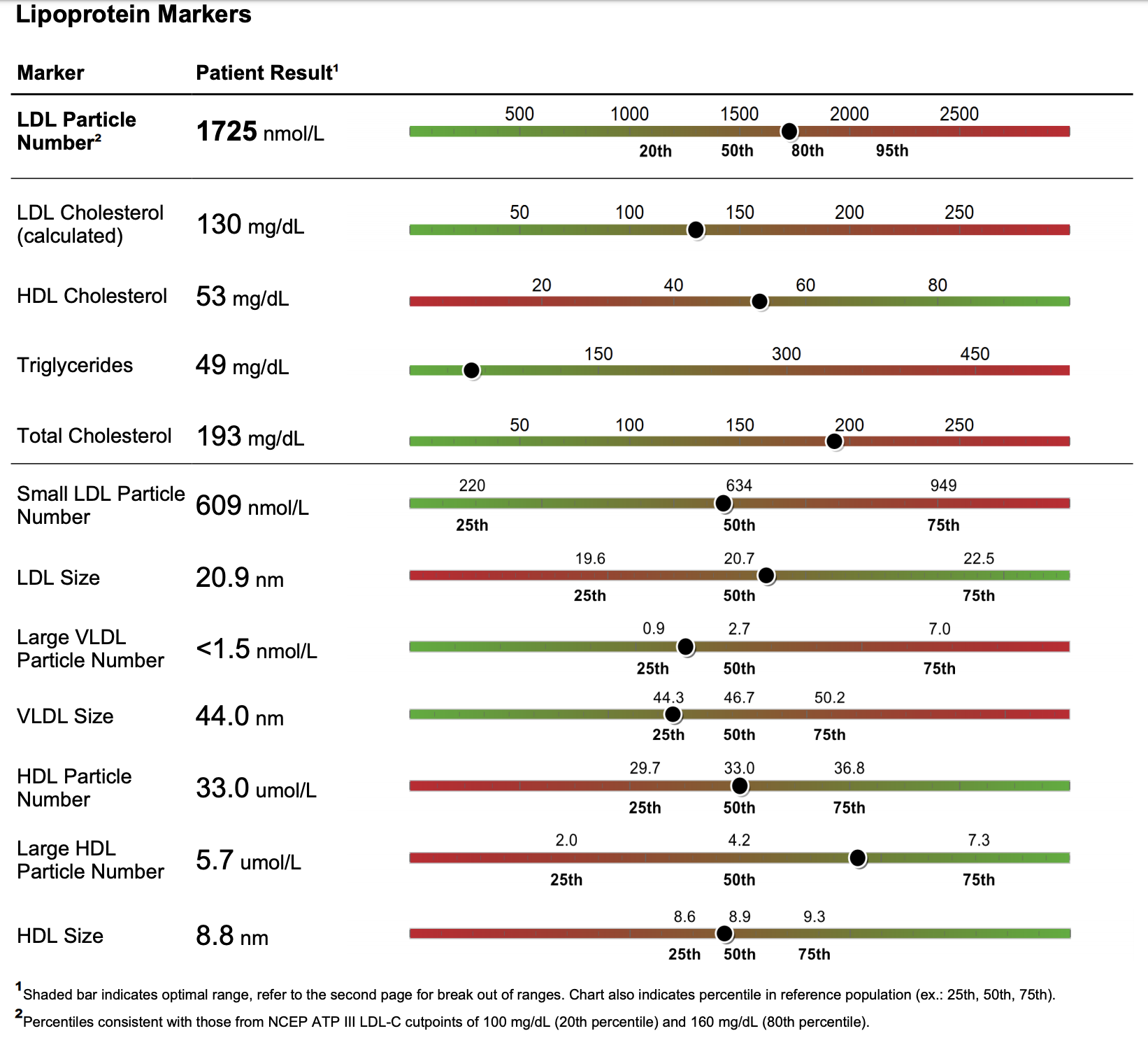
It’s a mixed bag. Obviously trigs are great and HDL is ok and trigs/HDL is quite good. But LDL-P is pretty woeful (though an improvement on late-2017) and as I read it the particle sizes aren’t great.
Any thoughts? Does this tell us anything?
ctviggen
(Bob M)
#29
If your CAC score is zero, those numbers are useless. LDL-p could be because you are using more LDL for energy.
I have extremely high Lp(a), but a CAC score of zero. If Lp(a) is not causing calcification (and I’ve had very high Lp(a) scores for the last 5+ years - probably my entire life though I never had them tested until the last 5 years), then how is it killing me? Similarly, if you have “high” LDL-p, but a zero CAC score, how is LDL-p killing you?
gabe
(Gabe “No Dogma, Only Science Please!” )
#30
I’m no biochemist, so I don’t pretend to know one way or the other, which is why I ask. However, the calcium score (which I did 2 years ago, so I’m not due for another for a while) only tells you where you’re at now. So, a little thought experiment: if someone had been on keto all his life and then he switches to SAD and gets a calcium score of zero 18 months later, does this tell you that he’s going to be fine 2 years from now? 5? 10?
Because of this, I see the calcium score as a solid waypoint, but I diverge from you in that I believe the other scores are, to varying degrees, useful in giving you more immediate feedback. For instance, your trigs, it seems to me, will definitely vary in accordance with your diet. Your inflammatory biomarkers like CRP are good indicators, I think, of how you’re doing.
The trouble is, there’s a lot of obfuscation around nutrition. When you point out to someone eating low carb that their LDL is high, they’ll point to trigs/HDL and tell you to get an advanced lipid profile done to check LDL-P and particle sizes. OK, so then you go get the NMR done and your LDL-P is sky-high (mine was actually in the 95th percentile last time) and your particle sizes aren’t “large and fluffy” like the experts say they should be. No disrespect to you Bob, but then you hear the sorts of things that you just said – “well your CAC is fine, so don’t worry about any of it.” You could have an LDL-C of 700 and people on these forums would tell you to forget about it.
I don’t buy it! So I’m wondering what this NMR tells me about my current state of health. Any ideas?
gabe
(Gabe “No Dogma, Only Science Please!” )
#31
I have, actually, but not that much recently. Recently I put on a couple of kilos, so last week I did intermittent fasting for a few days (basically delaying my first calorie until as late in the day/evening/night as I could) and rather enjoyed it. Got past 9pm one of those days, for a feeding window of like 3 hours. I’ve also temporarily quit alcohol and milk, and decidedly no out-and-out carb cheats, and in just a week and a half I’m back at my Phinney weight.
May do some IF again soon, though I do enjoy my morning coffee with heavy cream in it. I never thought an Americano with some frothed HWC in it could replace my cappuccino, but by God I think I’ve pretty much done away with my need for half & half!
Sorry it’s taken me so long to reply, but to answer this question: I read Body by Science nearly 2 years ago, I think at the suggestion of someone on these forums, and it convinced me that cardio may feel good, but you can achieve the same results biochemically with high intensity training, with the most efficient such training being single set to failure resistance training. I’m no Arnie, but I maintain superb blood test results and I effortlessly maintain my Phinney weight with just low carb eating combined with the occasional 15 minute gym session doing one set of 3 compound exercises (lat pulldown, chest press, row) on Nautilus machines to minimize the chance of injury and maximize the efficiency of the workout.
Cardio is detrimental because you’re wearing and tearing your joints and putting you at risk of injury. I live in NYC so I walk something like 60-80,000 steps per week (maybe 50km) just through incidental exercise, and most of that is brisk walking, and I injured myself riding Citibike last year, plus I haven’t got the best joints for a guy in his 30s, plus one of my knees is particularly challenging after a dislocation 20 years ago. I think the only thing I’d want to really add to my regimen is some HIIT on the bike, perhaps 20 mins of that twice a week; I was doing that until a few months ago but it became clear my knee didn’t like it.
PaulL
(You've tried everything else; why not try bacon?)
#32
I’ve lost all my links, so I can’t point you to the study at the moment, but David Diamond, in one of his lectures (I believe is the “Myth of Cholesterol and Heart Disease” one), gives a reference to a study done in the 1960’s on people with familial hypercholesterolaemia. The pattern of heart disease is striking: about 50% develop it, while the other 50% or so never do. The thing all the people with FH and heart disease had in common was genetic variations that made their blood much likelier to clot, primarily variants of fibrinogen and factor VIII. (Of course, the glycation of haemoglobin is also a factor, but that’s something we can improve by eating a ketogenic diet; genetics is a tougher deal.)
Ravnskov and Diamond have now actually proposed clotting abnormalities as the prime cause of cardiovascular disease. In particular, if the vasa vasorum gets damaged, it causes damage to the coronary arteries served by it. They posit that such damage actually occurs fairly frequently, and it’s only a problem when the rate of damage exceeds the body’s capacity for repair (in which cholesterol figures significantly).
I wouldn’t call a CAC scan useless as an indicator of risk, however. It is, of course, primarily a measure of damage, but it does appear that useful 5-year and 10-year projections can be derived from it, particularly if the patient has multiple scores, to establish what the trend is.
BuckRimfire
(BuckRimfire)
#33
I’ll agree with the walking as cardio! I like HIIT but I also like long walks and 3 to 6 hour sea kayaking days, which are usually at an effort similar to a fast walk.
I enjoy bike commuting, but I agree that it’s probably a major health risk!
BuckRimfire
(BuckRimfire)
#34
Not sure if he gave the reference, but he’s on the Diet Doctor podcast episode #27 (last month) and he talked about FH there, too, as well as several other subjects (statins, in particular). That is a good podcast series, IMHO, and it was a great episode.