
Thank you for this. There is so much nuance and possibility lost when we reduce everything to two sides and feel we need to pick a side and fight for it.
It's over - Ivor Cummins discusses the data (Let's stick with COVID) - this title got UNfiddled
FrankoBear
#123
No, I don’t think so Doug. Not everything. Especially not after this enlightening discussion. The dry tinder presentation might be argued, as it has.
The other material I do, at the moment agree with, in the context of having absorbed other interviews and expert opinions, so I can understand some underpinning knowledge that Ivor does not dive in to and possibly might take as more common knowledge than it is.
I try to temper things by triangulating my YouTube viewing (as part of my PhD studies) with the video presentations by Dr. John Campbell who flows more in the main stream. His presentations, especially when it comes to mask wearing contradict, in part, what Ivor presents and I understand the difference in opinion.
You can tell I mainly am bothered by the attack on Ivor as a messenger and the turning of some of the pack (I can feel the eyes of quite a few readers that are not commenting) on someone who once was a respected leader. My assessment still, is that was/is unjustified. I’m still struggling with it. It may take some time to catch up with the pack.
gabe
(Gabe “No Dogma, Only Science Please!” )
#125
Not at all. It’s actually rather likely that we will never get a mass covid outbreak in Australia again. Depends on the vaccines that emerge in the next few months. My understanding is that the likelihood of quite an effective vaccine is very high.
No. We have quarantine for 2 weeks. The quarantine system is extremely effective.
The virus is not “wild” in Victoria. It was wild in NSW, and now we’ve had 1 case of community transmission since September 7 (and even that may end up being traced.) We’ve effectively eliminated the virus for the 2nd time in NSW, as I expect VIC will shortly.
You’re just not right about this mate.
PaulL
(You've tried everything else; why not try bacon?)
#126
If you don’t want to present evidence in favour of Ivor’s articles and videos, that’s fine, but such a strategy won’t help me understand his points and perhaps accept them, when they seem irrational on their face.
For instance, I am not convinced that 80% of the populace already possessed antibodies to this virus before the epidemic even started. I saw where Ivor asserted that in the video, but it is not clear where he found the data to support that notion. The only other sources I have encountered on this matter were clearly speculating, not presenting actual data. So, until someone provides those data, I will remain puzzled and not yet convinced.
FrankoBear
#127
Gabe, mate, that’s quite a definitive statement. I thought we were in “time will tell” mode?
Last I checked Australia is on Earth. People are the vectors. The virus is very infectious and Australia won’t be closed off from the rest of the world forever. It’s not closed off now. In places the SARSCoV2 virus has joined the endemic respiratory viruses.
I applaud your positivity and further wishful thinking on vaccines. My understanding is the likelihood of quite an effective vaccine is low. We should share our resources.
There were these(1) comments by Professor Ian Frazer about the challenges in developing a corona virus vaccine. There are challenges with immune system response to the virus in the primary entry point of the upper respiratory tract.
“One of the problems with corona vaccines in the past has been that when the immune response does cross over to where the virus-infected cells are it actually increases the pathology rather than reducing it,” Professor Frazer said. “So that immunisation with SARS corona vaccine caused, in animals, inflammation in the lungs which wouldn’t otherwise have been there if the vaccine hadn’t been given.”
But I guess bacterial intranasal and pharyngeal vaccination does have some success, but generating a vaccine against a virus is a further challenge. So, I remain a bit more pessimistic than you on that. I’m also a bit tainted in my view from clinical experience. The gap between our outlooks can be bridged by hopefulness on my part.
Yes. We have quarantine for 2 weeks. The quarantine system has been very effective. We are dealing with humans. Now, what did you say earlier about the outbreak in Victoria? It was a quarantine breach.
Also, what is the incubation for the viral disease to infected disease state? And what is the duration of the infectious state?
It’s not fool proof. And as you clearly point out, there are Covid deniers about.
Maybe the term ‘wild’ is confusing? The virus is outside of quarantine and in the community in Victoria. (e.g. 0 days since last local infection) (2)
Fair enough I may not be right. I think we have established that “time will tell”. But equally I am not just not right.
(1) https://www.abc.net.au/news/health/2020-04-17/coronavirus-vaccine-ian-frazer/12146616
(2) https://www.abc.net.au/news/2020-03-17/coronavirus-cases-data-reveals-how-covid-19-spreads-in-australia
anon81060937
#128
I’ve heard from a family friend that’s testing a vaccine. He said the vaccine clots the blood just like the live virus. This seems like a gamble in regards to effectiveness.
MarkGossage
(bulkbiker)
#130
This one is suggestive that it could be more than was originally thought… although possibly not 80%. That number was probably used logically to explain the 20% who caught it.
SteveTheShark
#131
I just want to chime in here that when Ivor says “it’s over”, that means it’s no longer a pandemic, not that COVID no longer exists. I think it’s hard to argue it should be called a pandemic when hardly anyone is dying or is hospitalized any more.
Without the media hysterics, would any of us even know something unusual was going on? I’m beginning to doubt it.
petert
(Peter)
#132
If a vaccine ever arrives. Vaccines are not guaranteed - there’s never been a SARS vaccine, so there may not be one for this variant, or there may not be one for this variant in the next few years.
Either way, it’s not a given outcome, and shouldn’t be planned for as if we’re just holding out until it inevitably arrives. Especially given the (quite reasonable) suspicion around a vaccine that is developed at “warpspeed” and with possibly irregular testing.
Yeah, they were, but they’ve departed from the COVID threads currently to tend more carefully to their chickens.
Oh Lordy… (Particularly relevant thread for it, though.)
PaulL
(You've tried everything else; why not try bacon?)
#133
Interesting and very hopeful article, although
. . . they were all quick to note that this is speculation. Formally, the clinical implications of the pre-existing T cell reactivity remain an open question. “People say you don’t have proof, and they’re right,” says Buggert, adding that the historical blood donor specimens in his study were all anonymised, precluding longitudinal follow-up.
There is the notion that perhaps T cell responses are detrimental and predispose to more severe disease. “I don’t see that as a likely possibility,” Sette said, while emphasising that we still need to acknowledge the possibility. “It’s also possible that this absolutely makes no difference. The cross reactivity is too small or weak to affect the virus. The other outcome is that this does make a difference, that it makes you respond better.”
Weiskopf added, “Right now, I think everything is a possibility; we just don’t know. The reason we’re optimistic is we have seen with other viruses where [the T cell response] actually helps you.” One example is swine flu, where research has shown that people with pre-existing reactive T cells had clinically milder disease."
So it appears that the conclusion to draw is that there may be reason to hope, but the implications of the data are not yet clear.
PaulL
(You've tried everything else; why not try bacon?)
#134
I’m very glad for you, that in your area things have worked out so well. They have not, in much of the rest of the world.
This reminds me of my father’s complaint that the authorities had gotten all worked up over nothing after one of the big storms that hit the northeast U.S. a decade ago (not Sandy, but one of the others) blew past his area without much damage. Then he discovered aerial photographs of roads washed away and buildings smashed in a part of New England near where he grew up, and where we have family. It brought the seriousness of that storm home to him, in a way that my admonishments (not to mention photos of downed trees in my area) did not.
DodgeBoys
(Art)
#135
If that is what Ivor is saying, then he’s wrong there too.
Just curious - why would you say that? A large majority of the world’s population hasn’t been exposed to the virus yet, and the death rates are not to where we can truthfully say “hardly anyone is dying or is hospitalized any more.”
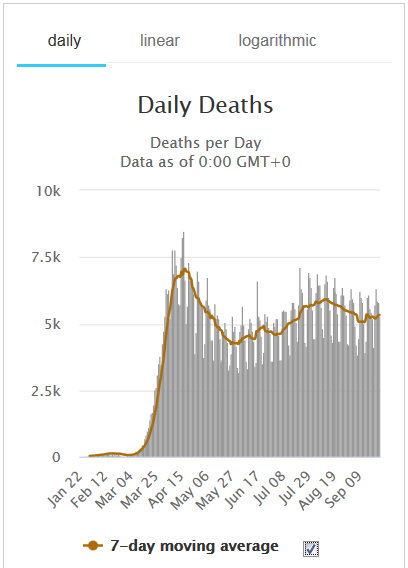
Deaths went up to an initial and highest-thus-far peak in April, down into early June, up to a lesser peak in July, down into early September, and may be now going sideways or back up some. The current death rate is 75% as high as the most-deaths-thus-far period in April.
The heavier-populated northern hemisphere is going into Autumn and Winter, times of perhaps greater virus activity. There is a lot we don’t yet know, but less than half a percent of the world population has tested positive, and even with a large multiple of that representing those who’ve been exposed without symptoms or who weren’t tested in any case but still were exposed, there’s still plenty of room for ‘immunity’ to not be that big a thing overall.
MarkGossage
(bulkbiker)
#137
Well it’s so far added about 7 days worth of extra deaths to the global total as over 150k people died every single day before COVID so an extra weeks worth of deaths… hardly a fearful pandemic and its been around for over 6 months.
We also of course don’t really know how many COVID itself has actually killed as opposed to those with various co-morbidities who may well have died anyway this year. Yes there have certainly been excess deaths (and there likely will be even more from the after effects of lockdowns etc) but with the loosening of autopsy requirements and the ability to add COVID to a lot of death certificates it’s very hard to tell.
One thing it has certainly highlighted in the UK for example is how appllingly bad our recording of deaths is.
Madeleine
#138
I had never thought of it like this! Actually, I probably wouldn’t know (personally), just like I didn’t know until this morning that 1.5 million people died of ----- in 2018 and 2019. It’s an infectious disease, and not the flu. @petert, if you don’t instantly know what I’m talking about then @SteveTheShark may have a point.
GME
(GINA )
#139
I would not know anything was going on if not for all the media hype. Oddly enough, an unusual number of ‘friends of friends’ have died in the past few weeks, but not with or from covid. Heart attacks mostly, which makes me wonder if they had gone without medical care because either they were afraid of being infected, or doctors/hospitals were too hard to get into because of the lockdown. Or who knows what other reason.
ETA: Maybe this is the reason, or part of it. Our air has been terrible for most of the past several weeks.
Justin_Jordan
(Justin Jordan)
#140
Now go and look up how many tuberculosis deaths happen in the first world, since that’s presumably what you’re referring to.
FrankoBear
#141
Paul I do like your comments. I learn a lot from looking at things from your point of view. You make me think, and in doing so I am able (you enable) me to get closer to understanding.
An epidemic dissipates from:
1. killing off all the hosts,
2. infecting enough people who recover, so that herd immunity can protect the rest,
3. isolating the infected population stringently enough to prevent its spread into the remainder of the populace.
- self limiting, self destruction; biology of disease immune to human interference. The pathogen is successfully infective but too destructive. A terrible epidemic that kills off hosts, vectors and pathogen alike. It is a major fear at the start of the epidemic. Thankfully it has proved to be not so severe as that instinctive fear would have us imagine. It’s worth mentioning as we can observe that fear is a consequence and a driver of human behaviour during a pandemic. It also speaks to the evolution of the virus itself with mutations favouring the virus’s existence, where the lesser destructive, but still infective forms will predominate over time. Unfortunately, at the start of an epidemic we are dealing with virus forms that cause fast spread, severe disease and death.
- the development of immunity. The development of individual and population immunity. The modulation of individual immune response. That part is so relevant to the ketogenic diet perspective and the diet’s effect on the human inflammatory response. I find this area very interesting to dive a bit deeper into and with that discussion elucidate some deeper understanding to mitigate concerns.
- protection of the vulnerable. Human instinct. We try to look after each other within our social groups. But how? It’s a highly infectious respiratory virus spreading through a species of social animal that we can observe, in many cases, need the dynamics of groups (families et al) for a healthy life. This area we can talk about vaccination, I think. Vaccination of the healthy who are in contact with the vulnerable, for their vaccination response may be adequate to create immunity. And to attempt vaccination with consent of the vulnerable (e.g. the frail, co-morbid elderly) to attempt to stimulate immunity in them - which takes us to how do we prepare this group for vaccination to get the best result? Possibly I suggested immune system supportive dietary approach could be considered? But the top is off this can of corona, as we try and identify the ‘vulnerable’ group, or the flavours of vulnerability. The data on severity of disease and death in patients with comorbidities such as metabolic disease indicate that any insulin resistant person may have a tougher time of coping and healing from this viral disease infection. I’m not sure of the exact numbers, but will chose 70% of USA-like dietary communities may be in this group… and that heads us toward mandating whole of population vaccination and social or legal consequences for those that do not vaccinate. Crikey, that discussion would be best pushed back to other social media fora, I think.
Point #2 is the one where I think there may be a diverse opinion to knock back and forth over the net (the Internet). There is concern that the normal immune response may be inadequate and that re-infection may be common. I think the limited data on that has shown that it is rare for a recovered infected person to become re-infected, and the observations that suggested that concern have had faults in measurement or testing, rather than demonstrating true re-infection. That being said, it is recognised in immunobiology that re-infection is possible in individuals that are unable to mount an adequate immune response to the disease. So, people who are immunosuppressed may develop subsequent infections.
As an aside it is very interesting that one of the therapeutic tactics is to create pharmacological immunosuppression at the anti-inflammatory level using dexamethasone at exactly the right point in the disease progression. I wonder if people whose lives are saved by that intervention in the acute phase, may be more susceptible in the future to re-infection. Probably not, as I understand the immunosuppressing corticosteroid dexamethasone is not prescribed as an ongoing treatment, it is used to suppress the cytokine storm and resultant inflammatory cascade. Right here in this thinking about inflammation within immunity and immune responses, is where I wonder if nutritional ketosis (maybe through fasting), or induced ketosis through supplementation with exogenous ketones would have some beneficial effect?
I think in this comment we have a pressure point. That being not knowing if the infection will return unrestricted based on the available antibody test data that shows that only a small percentage of the population (single digit percentages) have been able to generate antibodies to the infection. And then using the presence of antibodies data as the proxy, or the measure, of herd immunity.
That’s where the interview (previous post) and discussion that Ivor has with the immunologist is an interesting (and hopeful) deeper dive with some immunology science as it’s core. It may provide some demonstration about the 80%-ish extant immunity in a community? They discuss innate immunity, T-cell immunity, corona virus viral proteins^, cross immunity from exposure to “common cold” corona viruses, and antibody generation specific to SARSCov2. I don’t think they talk about serum transfusions of recovered patient’s blood to severely infected patients, but that therapy has been mentioned in other media reports. We can see there is, once again, more to it than just, in this case, antibodies.
I’m trying to turn this COVID19 ocean liner to discussion in context to ketosis, and leave Ivor to recover from the well intentioned (maybe?) character bashing he has received behind the ketogenic forum lunch shed.
^ @richard 's recommendation of microbe.tv is so excellent. Thanks Richard  I was watching the discussion between the microbiologists about the proteins that make up a corona virus and the variety of ways those proteins create different antigenic and resultant immune responses. I learnt that some animal corona viruses don’t have a haemagglutanin protein in their capsule and that can be a way of differentiating different types of corona virus. The ability to stimulate the agglutination (forming of clots) in blood is interesting as I think we have seen @anon81060937 raising it as a problem with vaccination development and also an undesirable consequence of the disease from natural infection.
I was watching the discussion between the microbiologists about the proteins that make up a corona virus and the variety of ways those proteins create different antigenic and resultant immune responses. I learnt that some animal corona viruses don’t have a haemagglutanin protein in their capsule and that can be a way of differentiating different types of corona virus. The ability to stimulate the agglutination (forming of clots) in blood is interesting as I think we have seen @anon81060937 raising it as a problem with vaccination development and also an undesirable consequence of the disease from natural infection.