I just visited a borderline T2 diabetic friend at the hospital after a stint was installed.
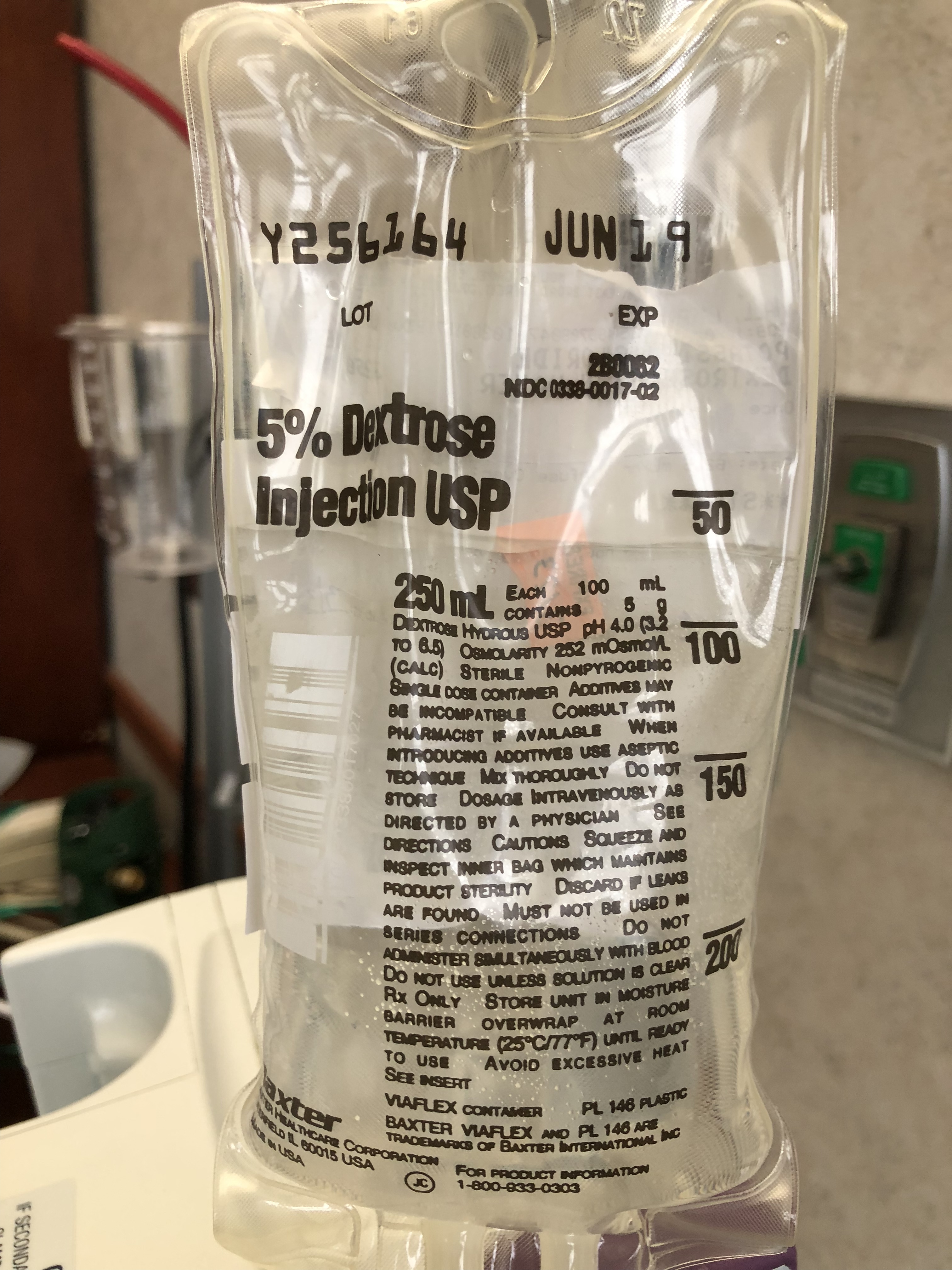
What are the reasons for putting him on a 5% dextrose (puke) drip? The cardiologist ordered it.
I’m blown away… and pissed really.

I just visited a borderline T2 diabetic friend at the hospital after a stint was installed.
What are the reasons for putting him on a 5% dextrose (puke) drip? The cardiologist ordered it.
I’m blown away… and pissed really.
= drug dealer??? I’m only half joking.
Could be easier to give IV dextrose than adjusting meds down to compensate for lower BG in the absence of oral food intake.
Some facilities may be experiencing the shortage of sodium chloride iv fluids, though I think the calories point raised above is a good one.
https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm585720.htm
Maybe…but my money is on they do it by practice because they think everybody needs nutrition after surgery.
When I had major surgery several years ago and a 2 day hospital stay, I requested everywhere that I could and in writing (before surgery visit at hospital, day of surgery check-in, and with my surgeon) “don’t give me sugar water IV drip, give me saline drip, only” and they followed my request.
I am not diabetic, though. (Which makes the sugar drip even more crazy, but that’s modern medicine for you)
Well, I asked around and it turns out he was low on potassium… so they injected the bag with some. Dextrose water was the delivery medium.
Bleh. They have a saline option. You have to specifically ask.
if your friend is not fat adapted, he needs calories from carbs. it is what it is. when a diabetic comes in to the hospital, they have to assume the patients have meds on board, including slow release meds. if he hasnt been there for more than a day or two, you have to appreciate that this is about an abundance of caution. if he was moderately healthy enough to tolerate some instability in his basic blood chemisties (including glucose) he wouldnt be in the hospital. let the drs and nurse do their thing, he’ll be home soon enough, and thats when it really matters what he takes into his body- when he is healing/ returning to health. right now is just crisis management.
I started keto soon after being diagnosed with type 2 diabetes. That was August 2018 and I continue to monitor my blood glucose randomly after meals and I am almost always below 120. I am 69 and my last doctor visit was advised that it’s best for me to maintain a BMI of 24.5 to 26 to help me sustain in medical crisis. But it occurs to me that I might best survive a medical crisis if I maintained fat burning. What do I do? Additionally, I continue to lose weight by eating Keto and am now at a BMI of 24.2. I know that I’m still insulin resistant because after foolishly eating a pint of blueberries I spiked my blood glucose to 167. A simple saline solution would get me by for a couple days but what if my medical condition required an extended Hospital stay? From what I’ve learned from Dr Phinney, I would have much more endurance if I maintained a fat burning mode.
This is much lower than most over the counter soft and even ‘health’ drinks even though it’s a glucose drip.