@ctviggen Yes, yes, and yes.
Wish I had more pre-keto data too.
Having exercised (cardio) daily for almost 30 yrs while eating LFHC (slowing gaining 25lbs and +4" waistline), I thought it was all just getting old. Didn’t realize damage was happening - until going keto.
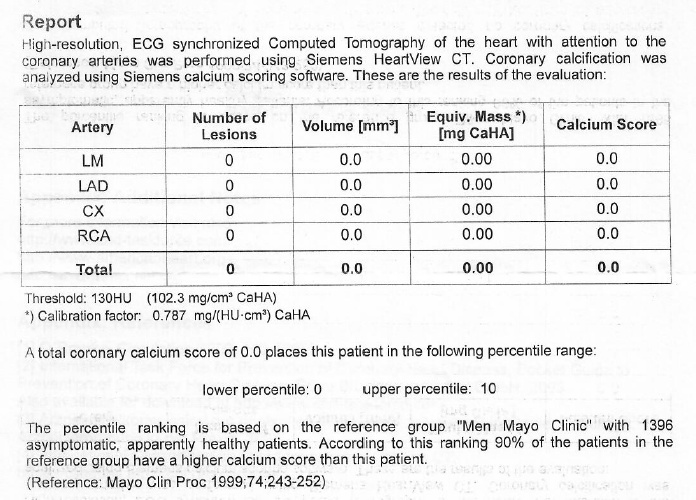
Upon restricting carbs, I started getting CT scans and my CAC scores were increasing steadily with each successive scan. Kind of scary.
I chalked it up to (= hoped?) calcification - reflecting a healthy, if not disconcerting, repair of prior soft plaque damage from all those decades of unrecognized inflammation.
Magically, my most recent CAC score (after 2+ yrs on keto) dropped sharply - although “magically” may involve significant K2/D3 supplementation. Sadly, have no pre-keto CAC scan results - a missed data opportunity.
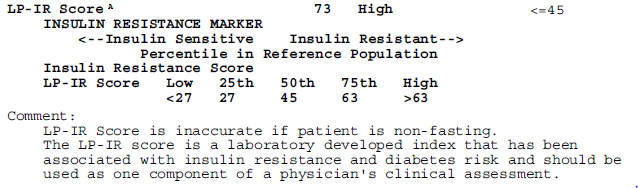
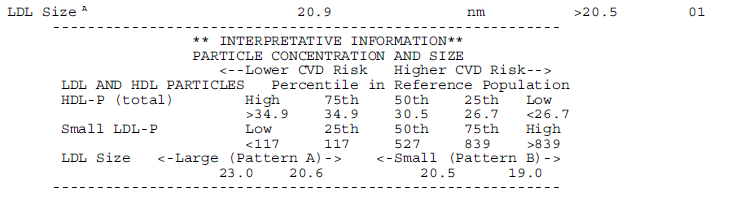
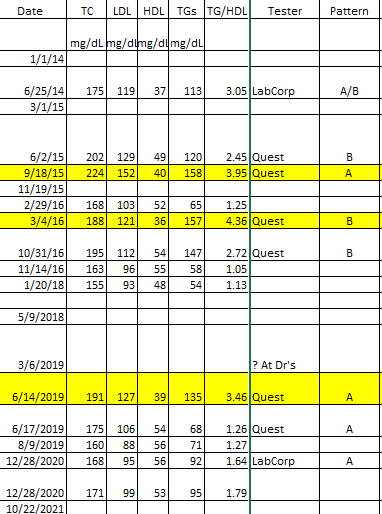
On the lipid side: latest HDL is 119 and trigs are 52. Deep in Pattern A territory, and LP-IR is <25 (below the chart’s bottom end, suggesting significant insulin sensitivity).
Regular exercise (HIIT strength + burst cardio), super low inflammation markers, and elimination of a range of pre-keto inflammation symptoms, all of which suggest keto is “working.”
BTW, eating ample salt and clocking in with low blood pressure, I also lost that 25lbs and came back to a 31" waistline, all while eating to full satiety on LCHF. Not a goal, just things that happened.
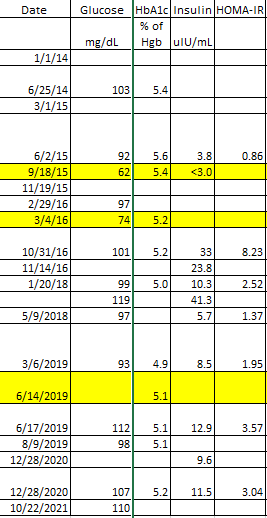
So back to insulin… It’s hard to get agitated about my typical morning glucose level now of roughly 100 mg/dL (had been more like 85 when I started on keto). These days, it meanders higher by as much as +20mg/dL post-prandial, then wanders back down to mid-90s. Safe to assume that’s what my liver and pancreas have conspired to produce.
But since I’ve never bothered having my insulin level tested, I can’t construct a HOMA-IR metric. To @PaulL’s point, context can be a rather important consideration when interpreting biomarker results.
So I’m going to continue assuming this all equates to a rather “insulin sensitive” profile - given everything else going on in this context.