
“my opinion” what I find is that in the Keto community there are a lot of opinions that come from presuppositions to support their position, a tendency towards dogmatic adherence to specific Keto principles, often without considering individual variations… Everyone is knowledgeable but the information comes from the same sources. I was this way for years! When I started Keto there were no products on the shelves marked Keto friendly we eat natural food from proteins, good fats and minimal carbs mainly from vegetables. I am a runner, cyclist and strength train for most of my life and still do to this day. I am a lean 68 year old man who most people say look like I am in my 50s. Even though I have done all of that for years I now have ASCVD. Obviously Keto has not stopped or slowed the progression for me after all these years because I have a CAC of 1114! On this forum people say “double down go carnivore!” Or, try K2, Niacin or all the other remedies that are suggested. Don’t get me wrong I am not being critical of this forum I asked them to give me there opinions and I am appreciative for that. But at the end of the day I have to make a decision going forward because I am at high risk right now. I have no physical problems and take no medications so to be asked to take a statin is very hard for me. That said, at this point my thought is to move toward a lower carb Mediterranean plan with a low dose statin. I know that probably isn’t a popular approach on this forum but it’s where I am at right now.
High CAC Score
In the end, we all make the best decisions we can with the available knowledge that we have. That is all we can do. You need to do what is best for you. It never hurts to gather info and hear other opinions, but in the end, we are not doctors. 
These are just my musings and I haven’t researched it, but I’m wondering, do statins actually stop the progression of calcium build up in the arteries?
Also, if you are a lean mass hyper responder, it would seem all you would need to do to lower your LDL would be to increase your carbs somewhat. It might be an interesting experiment to up your carbs a bit and see what happens to your LDL. That could prevent you from needing to be on the statin.
Minimal saturated fats could still be keto. You would just be using olive and avocado oils instead.
Good luck with whatever path you choose to take.
No panels not high before Keto. No family history of heart desease my mom lived to 93 my dad to 91. I am 68. I can see the images from the CT scan the plaque is significant. Under a doctors care now.
Very glad to hear this. Keep in mind generally that most males over the age of 60 will have an elevated CAC score, and while this number is important, less so over the age of 60. This is not your case, as your number is over 1000. Stacked with other markers could lead you to a new course or action, including diet. (high recommend) Not everyone that does keto and/or carnivore thrive. Please keep this in mind when searching for answers here. If you suspect it is genetic, then it makes sense to have your son checked out and course correct. Better to be proactive than not.
Wishing you nothing but the best in health.
I hear you brother! We hail from very similar age/phenotype/lifestyle profiles with generally similar results.
My (personal) view when it comes to meaningful carb-restriction is that the damage from systemic inflammation throughout the body is far worse - and often irreversible - than “clogged” arteries - for which we have all kinds of modern medical techniques to address (viz., resolvable “plumbing” problems).
I don’t mean to be flip or dismissive of CVD risks but, when picking my personal poison, I’d rather reduce risks of cancer, dementia, insulin resistance, joint erosion, organ damage, etc. if that trade-off entails a bit more arterial narrowing.
This, plus embracing the soft plaque-scabbing beneficial effects of calcification, inform my n=1 choices.
Best wishes! 
Here is another take to throw out there. In 2021 I was hospitalized with Covid Pneumonia almost died during my hospitalization I had two CT scans on my lungs that indicated minimal plaque in my arteries. Granted they were looking at my lungs but at that point my life was on the line I would think that if something was concerning the doctors would have tried to address it. So huge inflammatory issues from Covid plus I was treated with Remdesivir, Dexamethasone and Baricitinib. Wondering if Covid and the treatment drugs could of had an effect on the dramatic increase in my ASCVD and recent CAC score? Have no data to back it up but Covid and the drugs that were used were so destructive! I always tell my wife Covid pneumonia almost killed me and changed my life. Took me almost a year to feel some what normal. Just thinking out loud.
That’s some serious thinking, for sure.
Your body’s response to exposure to the corona virus speaks to a heightened inflammatory tendency - at least to that particular viral strain.
To me, this would inform my course of action going forward, i.e., by focusing first and foremost on anti-inflammatory protocols given the menu of choices and trade-offs.
To be clear, we know inflammation itself is a natural, normal, and essential body function. But beyond this point, it’s also the #1 source of most every (non-trauma related) ailment the human body faces.
You could be correct. I found this interesting paper that seems to back your hypothesis.
Not sure how relevant but I find it interesting regarding prolonged fasting and heart related issues.
Interesting. I find it disappointing that the experiment in some ways failed or at least was gravely dangerous because of dehydration and electrolyte imbalance. These are simple matters anyone could address at home while water-only fasting, and with common sense should not have occurred. … It puts the entire situation into a realm of potential fanaticism / eating disorder rather than a medically sound experiment.
And too bad he went back to being a vegan, wasting all that hard work to get healthy. 
Here’s the main graph:
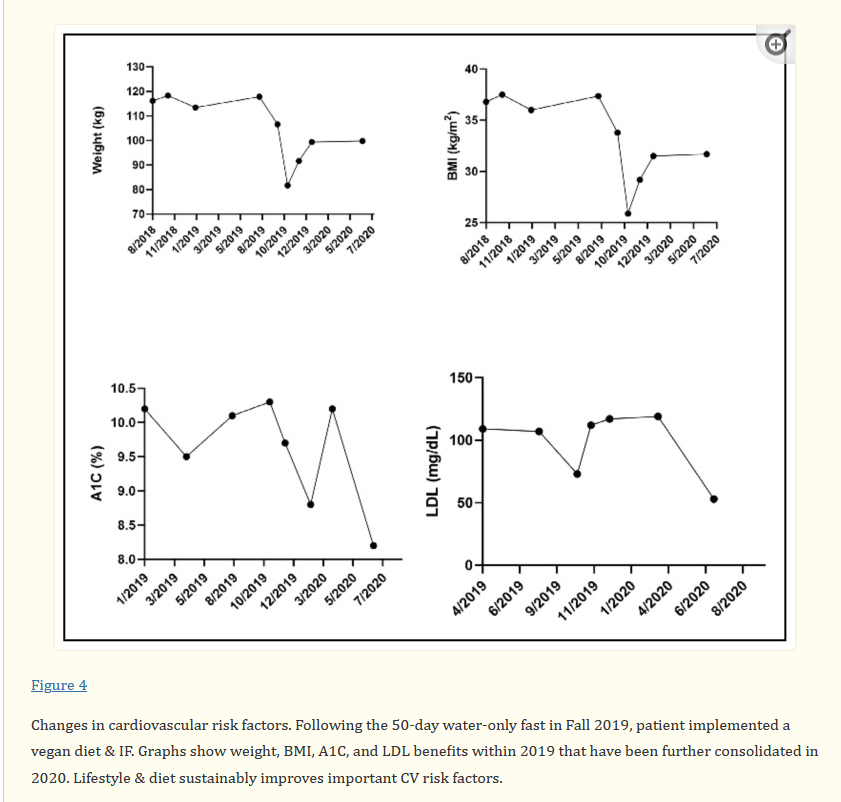
Although to try a 50 day fast when you can barely breathe. This was him: “His medical history includes hypertension, hyperlipidemia, type 2 diabetes mellitus on insulin, obesity, obstructive sleep apnea, depression, and asthma.”
Impressive he was able to fast like that.
Thank you for the paper. At least I know I am not the only one thinking along these lines.
Confirmation bias is everywhere.
I too was at the top of Mount Stupid (Dunning-Kruger Effect).
I get it. But the alternative could be worse. Your doctors will probably also give you a PCSK9 inhibitor as well. If the statin you are prescribed gives you problems (side effects), tell your doctor, and he will put you on a different one that hopefully has no side effects. Absent of other potential causes, I would most certainly stop keto. Ask your doctors lots of questions on the journey. Remember, the squeeky wheel gets the grease.
On a separate note, I was a former MTB racer for 17 years and then switched to road racing.
Dunning-Kruger Effect
Haha that fits me to the tee. Preached keto to everyone! I trained my son to fuel his body by being low carb and use ketones. He started racing MTB in HS and then started as a junior on a team racing crits he raced MTB, crit and road till he went in the Marines in 2019. One of his friends races ucipro now her name is Gwendolyn Gibson. As I said I am transitioning to a Mediterranean eating plan. Started the statin and already had to change because of stomach issues. Asking lots of questions.
Appreciate the post. Hopefully you still get to ride.
Gwendolyn I think won nationals? Yes, I still ride and average about 8000 miles per year. Still trying to get back to my best FTP of 355. I will never give up the fight. Still race, but only occasionally. We cyclists love to suffer (on the road).
Sounds great. Curious if you measured your macros while doing keto, and if so, how will you transition to a Mediterranean plan? I eat a lower-carb diet about 80-90% of the time. I rarely do fasted training rides anymore. I was given an Oura ring about 7 years ago and found out that I was undernourished. This affected my sleep, recovery, training, racing, and general wellbeing. Within two weeks of adding in more food, primary carbs, my world changed. Sleep score went up significantly, I recovered better, I could train better, and instead of finishing in the middle of the pack and being completely wasted for the next three days, I started to consistently podium. Plus, I was pleasant to be around and could relax.
I did measure my macros daily to make sure I was on target for carb, proteins and fats. As for my transition to the Mediterranean plan is going to be just that a transition. Incorporating foods I haven’t eaten for years like steel cut oats, beans, lentils, more fruits is going to take some experimentation for me. I slowed down after Covid in 2021, then knee replacement in 2022 but still walk every morning about 4-5 miles then ride about 15-20 miles along with strength training 4-5 times a week. I feel good and sleep good. Curious what is your age? What eating plan are you using now? What statin and dose are you taking?
Blueberries, raspberries, and blackberries are really good, especially first thing in the morning. They help with recolonizing the gut. 3-4 times per week I will alternate between each. 3/4 of a cup.
Perfect. Never give up. Our ability to maintain or build muscle becomes harder as we age.
I turn 60 soon. I was very fortunate to be exposed to endurance sports at a young age and have continued ever since. As of a week ago, my VO2max was higher than my age.
I started the keto journey about 15 years ago under the supervision of a medical doctor and a sports scientist. I measured everything possible. My focus is no longer keto but still lower carbs (grains) about 80-90% of the time. I also did IF and extended fasting. I no long do any fasting on purpose. The scientific literature on fasting in humans is still relatively weak. even Dr. Fungs says this. My focus for the last few years has been the gut biome and balance. I try to keep up a higher protein intake and shoot for a minimum of 1.6 grams/kg of body weight.
I have never been on statins and have no family history of CVD that I am aware of. However, on my wife’s side, it runs in her family. Please note I am not a medical doctor but someone who has read a lot. It also helps that my wife and both of her parents were medical doctors. Here is some information that I have glean over the years. The most common statin that most doctors start with is rosuvastatin (Crestor). If you cannot tolerate this statin, then a newer drug called bemedoic acid (Nexietol) can also be prescribed. Ezetimlbe (Zetia) is also used. These should help reduce ApoB. There are also PCSK9 inhibitors, which, when used together, are a powerful tool to help lower ApoB. Statins do not reduce Lp(a), but PCSK9 does in most patients, typically about 30%. When it comes to Trigs, if dietary interventions are insufficient and genetics plays a role, then there is a drug called vascepa.
I realize on this forum the very mention of statins is verboten, but they can and do work for most. The statins of the past are different than before. Have a look at the work of Dr. Allan Sniderman. He has been a research cardiologist for more than 50 years. Most of the experts/doctors that are mentioned are either not medical doctors (red flag) or have never produced any scientific papers. Or if they have, they have never been cited by others. In some cases, especially the YouTube doctors, they will cherrypick one small aspect of a study and proclaim this as the entire conclusion of the study, as most people will not read the study. This was done by a YouTuber who cited a study from Norway on hypercholesterolemia. All ages showed an increase in risk except the 60-67 age. He took the exception as the rule. There is no perfect diet. Anybody who makes that claim is a charlanin.
I’m not sure anyone’s doubting the ability of statins to affect lipid panel results. I think the question is, is that “work” necessary and beneficial. Does it meaningfully prolong life or healthspan? That’s where I keep coming up short. If the only thing statins change are numbers on a piece of paper, I’d rather just use some WhiteOut.