Background: I’ve been LCHF since July 2016, keto since about 2 months ago. Just had my CRP done, and it’s 0.99 (down from 2.2 in October last year.) High LDL-C and over cholesterol led the doctor and me to run an advanced lipid profile.
I’m slightly confused - my LDL-P seems high, HDL-P seems low, but then I have a low small LDL count which I know is good. Can anyone help with this? @DaveKeto@richard ? Anyone else? Would love your thoughts.
Best
Gabe
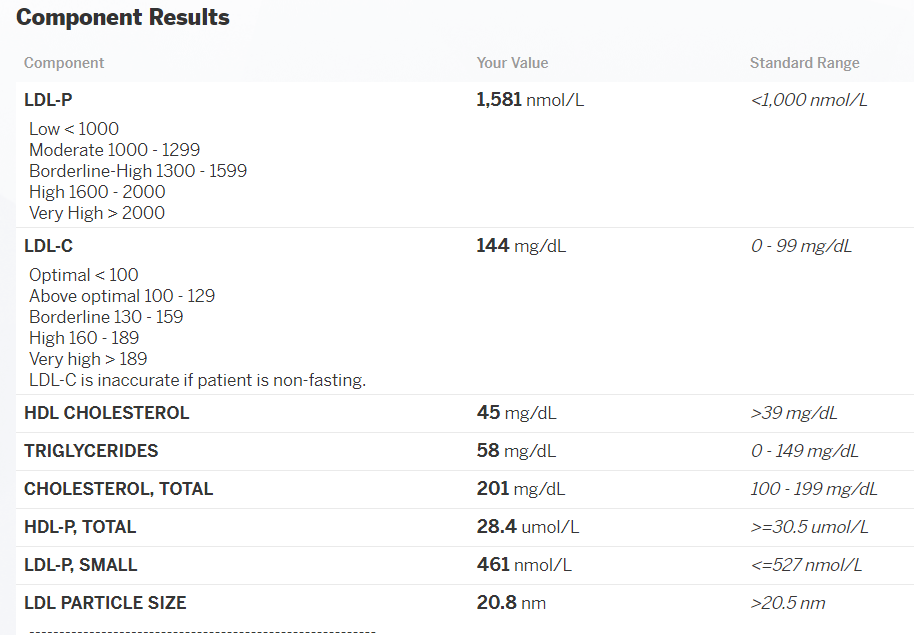
Component Your Value Standard Range
LDL-P 1,581 nmol/L <1,000 nmol/L
Low < 1000
Moderate 1000 - 1299
Borderline-High 1300 - 1599
High 1600 - 2000
Very High > 2000
LDL-C 144 mg/dL 0 - 99 mg/dL
Optimal < 100
Above optimal 100 - 129
Borderline 130 - 159
High 160 - 189
Very high > 189
LDL-C is inaccurate if patient is non-fasting.
HDL CHOLESTEROL 45 mg/dL >39 mg/dL
TRIGLYCERIDES 58 mg/dL 0 - 149 mg/dL
CHOLESTEROL, TOTAL 201 mg/dL 100 - 199 mg/dL
HDL-P, TOTAL 28.4 umol/L >=30.5 umol/L
LDL-P, SMALL 461 nmol/L <=527 nmol/L
LDL PARTICLE SIZE 20.8 nm >20.5 nm
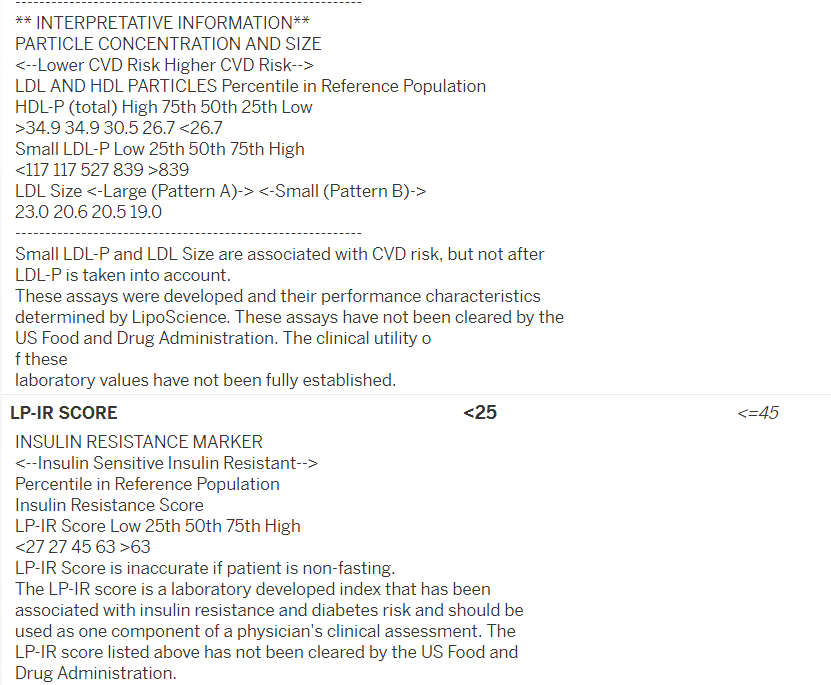
** INTERPRETATIVE INFORMATION**
PARTICLE CONCENTRATION AND SIZE
<–Lower CVD Risk Higher CVD Risk–>
LDL AND HDL PARTICLES Percentile in Reference Population
HDL-P (total) High 75th 50th 25th Low
Small LDL-P and LDL Size are associated with CVD risk, but not after
LDL-P is taken into account.
These assays were developed and their performance characteristics
determined by LipoScience. These assays have not been cleared by the
US Food and Drug Administration. The clinical utility o
f these
laboratory values have not been fully established.
LP-IR SCORE <25 <=45
INSULIN RESISTANCE MARKER
<–Insulin Sensitive Insulin Resistant–>
Percentile in Reference Population
Insulin Resistance Score
LP-IR Score Low 25th 50th 75th High
<27 27 45 63 >63
LP-IR Score is inaccurate if patient is non-fasting.
LDL-c and LDL-p vary depending on what you’ve eaten in the past few days (e.g. how much fat, how much food, etc) and how much exercise you’ve done.
Your HDL isnt low, but it isnt high either, but this is also influenced by diet. When I did the Feldman protocol I saw a 10 or so point increase in HDL in 3 days. Your trigs are also low (indicating youre using or storing the energy ehich is good). Insulin resistance also looks good.
Did you have any specific questions about the results?
Gabe, the formatting makes it hard to figure out all of what is exactly going on.
Lots of people know more about this stuff that I do, but HDL : Triglycerides looks pretty good, as above. Your raw triglycerides number is great. Normal is <150, yours is 58.
There is some disagreement about the ramifications of the LDL numbers and whether the particle size or number of small particles matters more. I don’t know enough to really say anything about it. In any case, from everything I’ve read, though your LDL-P seems high, I don’t think it’s high enough to necessarily worry about. I’d see what happens in the future while staying keto. Down toward the bottom of the report, it says, “Small LDL-P and LDL Size are associated with CVD risk, but not after LDL-P is taken into account.” There too, sounds like no need to panic, at all.
Your HDL-P is barely under normal range, and the total HDL number is in the normal range, hard for me to see any worries there.
Total cholesteral - normal is 100 to 199, you’re at 201. No problem. I also don’t know if it’s universally accepted as to how much weight should be given to this number anymore.
The Insulin Resistance Marker, LP-IR score at 25 looks very good, with less than 45 being the standard range, if I’m reading it right.
Your score at 25 looks like it’s below the 25th percentile for risk, so your risk for developing diabetes should be in the bottom quarter of the population (again, if I’m seeing things correctly, here).
Considering low LDL-p and low LDL-c are not good protective factors, and high LDL-p and LDL-c is not a good predictive factor I would say yes definitely total cholesterol is not great of a predictive/risk factor either.
Honestly a lot of these results are really a snapshot of what OP has eaten and done in the past 3 days which isnt very good for risk assessment.
The IR result and triglycerides at least are good, and the HDL may just require more saturated fat to help it. But other than that it all looks good imo.
Thanks, Siobhan. Now that we know it’s far from as simple a deal as the one ‘Cholesterol’ number, there’s a lot to learn, and it seems somewhat impenetrable at the beginning.
Thanks guys. I’ve screenshotted the results and pasted them below so it’s easier to interpret.
Yeah the reason I wanted this test was because my LDL-C was high on my lipid panel a few weeks ago. I wanted to show that my small dense LDL particle number was low.
LDL-P looks quite high, which is disappointing, but then SMALL LDL-P looks quite good. Not great, but good. Average LDL particle size of 20.8 also falls right in the middle of Patterns A and B, which is, I assume, not great, but good.
My HDL numbers are similarly meh.
I guess I’m wondering: am I interpreting this correctly? And I guess I’m also thinking: I’ve been eating really well. Why aren’t the numbers better?
Also – wondering how the LP-IR score is calculated?
LP-IR considers the density and size of various lipoproteins in one’s blood, and the numbers of them. There is strong correlation between patterns for those with insulin resistance and hence a greater chance of becoming pre-diabetic and then Type 2 Diabetic in the future, even if at present there is no loss of blood sugar control.
Considerations are:
The numbers of large-size VLDL (very low density lipoproteins).
The numbers of large-size HDL.
The numbers of small LDL.
Then, among normal-sized particles:
The numbers of VLDL, HDL, and LDL.
I can’t find the actual calculations for the LP-IR score. Some of the sizes of lipoproteins indicate they have triglycerides attached to them, and apparently this is a marker for increased chance of becoming pre-diabetic in the future.
Well it really depends on what you consider ‘better’.
For example, consider that LDL scores are largely influenced by what you’ve eaten and done in the past 3-5 days. Days!
Consider also that LDL-p has the primary job of transporting energy (triglycerides) and since the amount in your blood is low that this energy is getting to where it needs to go.
Consider also that HDL is also influenced by diet - I’ve had 2 blood draws done 3 days apart and there was a near 10 point difference.
So honestly besides low HDL which may be a fluke (or really just means eat more saturated fat) you seem fine.
Just to your point: the low HDL has now come out twice, once on a standard lipid panel and once on the NMR. More saturated fat? Or, as the doctors are going to keep suggesting, switch sat fat for mono? I’ve seen it said on some keto forums where people suggest switching saturated for unsaturated fats to deal with cholesterol remaining high on a keto diet.
Also, you said my LDL-P is low, but it seems, as I’m reading it, that my LDL-P is high. No?
Yeah, I’m also disappointed that the results (at least the ones I can see online) don’t have a more granular analysis of the lipoprotein particles.
Most disappointing, I suppose, is that the results are mixed. I’m not clearly Pattern A or Pattern B, I fall somewhere in between. So it leaves open the question of whether the doctors are right and whether I should be reducing saturated fats in favour of monounsaturates.
Okay, so it is consistent. That is interesting.
Monosaturated fats lower LDL (not necessarily good) and do nothing to HDL - no observable effect. Saturated fat raises HDL reliably - the effect we are going for.
You may find it interesting to watch Dave Feldman give a talk on “Lean Mass Hyper Responders” - you can find them on youtube or take a gander at his research on cholesterolcode.com
The point is that LDL - p or c - is not a causative factor of athersclerosis in itself. In fact, the foam cells which can develop into deranged plaque build up do not come from intake of normal, healthy LDL (into the arterial wall at all. They only develop when there is presence of bacteria, oxidized ldl, very old ldl, or glycated ldl (ldl damaged from glucose exposure). LDL in fact has very important roles within the body - it carries around energy, it can be absorbed by damaged cells to be used for repair, it transports fat soluble vitamins within it, and is an important part of the immune system.
So do we really want to lower something that has so many important roles, many of which we dont fully understand yet?
I am going with “probably not” on this one, especially because when we lower LDL via diet or statins we do not see a reduction in all cause mortality. In other words, even if by reducing LDL someone decreases their risk of heart disease, their risk for dying of an infectious disease, cancer, or diabetes (from 5% risk to 10% risk of developing diabetes) goes up compared to the placebo group.
What has been shown to lower risk of heart disease then?
Raising HDL (which can be done via increased saturated fat intake)
Lowering insulin resistance, basal insulin, and blood sugar to normal ranges
Lowering exposure to outside sources of Reactive Oxygen Species like smoking
And I meant to say “as (your triglycerides) are low” didn’t mean to imply LDL-p. LDL-p is the transporter, and triglycerides are the cargo. It is on and offloading cargo as it should, as indocated by there being no build up (trigs >100).
If you want to PM me, I can use it as a reminder to post resources and studies related to what I’m talking about when I get home. Hope this cleared up my point a bit!
I have listened to Dave and will read more of his research, but I would like to see other accredited medical/biochemical academic sources for these claims.
Okay! So I got home later than I thought so this is going to be rather truncated and I’ll follow up tomorrow.
First up: I should not have been so definitive about LDL-p because in all honesty it’s a new area of study (for us all!) and I was misremembering some info. Full disclosure!
HOWEVER! I do have reason to believe it isn’t much of a concern especially when paired with concordant LDL-c, such as the most at risk people having low LDL-c and high LDL-p, e.g. discordant pattern of LDL-c/p pattern. You’ll also notice in Dave’s research that LDL-p also goes down in response to increased fat consumption, just like LDL-c does. In fact it goes down at about the same rate. Some food for thought for sure.
That plus the fact that normal LDL in itself does not contribute to foam cell formation…
Surprisingly, native LDL is not taken up by macrophages in vitro but has to be modified to promote foam cell formation. Oxidative modification converts LDL into atherogenic particles that initiate inflammatory responses. Uptake and accumulation of oxidatively modified LDL (oxLDL) by macrophages initiates a wide range of bioactivities that may drive development of atherosclerotic lesions.
So what that is saying that what’s involved in athersclerosis isn’t “native” unmodified LDL but oxidized LDL. This is part of why healthy LDL that you have a lot of (high LDL-p with concordant LDL-c) doesn’t bother me very much, because that isn’t one of the triggers for athersclerosis. It is what causes glycation (excess exposure to glucose), oxidation (many factors, but external ROS is one), and age (abnormally high trigs as a result of excess carb consumption and insulin resistance) that is the issue here - not the LDL itself.
It isn’t only oxidized LDL though that can be taken in by foam cells… any modified LDL will do (very old LDL, glycated LDL, etc). You can just look up what scavenger receptors take in for more info on that part.
Here’s another part…
and scavenger receptors (SRs), that internalize apoptotic cell fragments, bacterial endotoxins, and OxLDL, leading to lipid accumulation and foam cell formation [2].
In other words it isn’t high LDL-p that is kickstarting the whole process, it’s damaged LDL (oxidized, glycated, or just old) that starts you down the road of athersclerosis. Can you have elevated LDL-p for damaging reasons? Indeed yes, as they even outright state here that with people with discordant LDL markers, LDL-p is a better risk factor
And of course high LDL-p can also be associated with insulin resistance (if paired with high triglycerides, and very low HDL), but also we see high LDL-p in lean mass hyper responders who have otherwise fantastic metabolic markers - and indeed Dave has demonstrated that this number is highly fluid (inducing a 1000 point drop in 3 days for particle count) suggesting there is a lot more to the story than might initially appear to be the case.
As for saturated fat and HDL:
Upon changing from high to low intake of saturated fat and cholesterol the mean HDL-C decreased 29% from 56 +/- 13 (SD) to 40 +/- 10 mg/dl,
However, when compared with the saturated diet, the synthetic rate of apoA-I was reduced by 26% during polyunsaturated fat feeding.
Monosaturated
Note that Olive oil ended up not even changing HDL 1% from baseline
but, as was reported by other investigators (14, 18, 19, 31, 32), the high MUFA diet did not affect the levels of plasma HDL fractions.
(As in didn’t raise or lower them)
https://www.karger.com/Article/Pdf/381654
This has lots of interesting stuff in it regarding LDL-c and all-cause mortality, more specifically that for men it is a U shape when it comes to mortality risk (extremely low and extremely high linked to more mortality) meanwhile with women it is an inverse correlation - higher the LDL the less they die. If it’s an issue of high LDL-c why don’t women experience the same thing as men do? Mystery upon mystery.
Here’s another showing correlation of mortality and cholesterol in men and women…
So, hopefully this isn’t too all over the place… Maybe you already know a lot of it, or there’s something I really missed or something. Just let me know. I kind of attacked this haphazardly so it may be sort of wonky at the moment. Sorry!
Basically, what I’m trying to say here is that with athersclerosis in order to even start you need oxidated or otherwise modified LDL. High amounts of normal LDL simply isn’t going to cut it, because this won’t initiate foam cell formation, which - in deranged states - ends up developing into a deadly state of disease.
If there’s anything I wrote here that’s confusing or you’d like more info on let me know. A lot of this is simply from reading through Therapeutic Lipidology and Clinical Lipidology so it’s hard to pull from them to post here.
EDIT: Almost forgot. Ivor Cummins has great stuff as well, especially check out 28 minutes in forward. That is the big risk factor I would be concerned about.
EDIT 2: This post is a straight up mess, but I don’t really have time at the moment to make it prettier. I’m hoping you’ll at least find something interesting here that can be of some use, or at the very least ask questions so I can respond to them point by point which I do better with.




 Now that we know it’s far from as simple a deal as the one ‘Cholesterol’ number, there’s a lot to learn, and it seems somewhat impenetrable at the beginning.
Now that we know it’s far from as simple a deal as the one ‘Cholesterol’ number, there’s a lot to learn, and it seems somewhat impenetrable at the beginning.