about Sweden - Yeah, I don’t know… I think time will tell. There are immunologists who are making a strong case that our previous exposure to different corona viruses are helping our immune response, which means we can’t really know who is immune by using COVID-19 antibody tests - so basically it’s hard to know if Sweden essentially made an investment in the future, reducing the death rate in next season’s flu/corona season. In late May, Norway issued a statement saying that their lockdown was a mistake, that it didn’t change the trajectory of the virus.
It seems to me that one thing that we’ve all forgotten is that the initial idea was to flatten the curve, not to stop the virus. I don’t think anyone actually thinks that we can stop the virus. Maybe a vaccine soon? but those take time and in the meantime - sadly - COVID 19 will take many lives as it circulates among the population. Like the flu that’s now around (which apparently is very close to the 1918 Spanish flu?!) its devastation slows because we develop immunity with exposure.
My concern is that with continued shutdowns we’re doing real harm to an entire generation of children. Months indoors, paranoid about hygiene, no exposure to the mix of pathogens that actually help build our immune systems* and with minimal social contact … this may show up in really unhappy ways down the line.
Has anyone seen reports that immunity may only be 90 days or less lately? I read this in a news feed somewhere (sorry, cannot find again so don’t know if this is accurate or false or even measurable yet) and haven’t seen much since on it as I spend minimal time online.
If the virus does keep changing, or immunity isn’t lasting, what could be a proactive response then?
Norway is sitting there with ~1/12 the per-capita deaths of Sweden. Pretty hard to argue with that.
That stuff from Norway was over 2 months ago, and made some incorrect assumptions about the transmission rate of the virus - in the time since we have seen just how fast cases can multiply. In that one report, it was also assumed that Norway could have achieved essentially the same results by taking other “precautions to stop the spread.”
Rationally, that is greatly in doubt. Norway has done hundreds of thousands of tests, and only 2.5% of people there are showing as positive thus far. Norwegians are fairly calm and compliant with gov’t policies, like Swedes, and it all does come down to the behavior of people, but I don’t think Norway is still trying to claim they could have done just as well without people staying home.
Sweden itself has slowed the virus spread dramatically - it’s only up to 12.2% positives now. Yet the gap between it and Norway is enormous. Thus far, Norway’s peak in new cases was on March 27, while for Sweden it’s June 24.
The common cold is a coronavirus, for example, and we really just don’t know about immunity for SARS-Covid-2. While personally I think “a vaccine by the end of the year” is probably silly, we do have over 6 months in already since the new virus appeared. So perhaps a meaningful chunk of the time we have to wait has gone by. If so, then Norway has obviously done pretty well. If we do get a vaccine “fairly soon,” i.e. this year or next year, then Sweden will be in the place of saying, “Now we have a vaccine, and if we’d done differently, we could have had 1/10 or 1/12 as many deaths…”
Yes, it’s possible. I wasn’t meaning to compare Sweden and Norway specifically but I was just interested in the lockdown comments from Norway. Sweden had a higher per-capita death rate going into COVID and I think probably other factors which (or may not?) figure into the numbers.
There are so many unknowns and I’m not particularly anti-lockdown but I’m afraid we’re so obsessed with lockdowns that 1) we’re not truly protecting people from COVID death and complications (by addressing the co-morbities, in particular insulin resistance/metabolic syndrome) and 2) we’re not really looking at the costs - to our children in particular - of shutdowns.
What is interesting is how this virus effects people differently in that they have very very mild symptoms where taste buds and olfactory nerves go dormant temporarily and a little dry cough but that’s it, they really don’t feel that ill and get over it pretty quick?
I wonder if that has to do with viral load (virus particles per milliliter) and it being more like a immunization and inoculation rather than a threat which is what a vaccine is supposed to do?
References:
[1] “…We begin our history of vaccines and immunization with the story of Edward Jenner, a country doctor living in Berkeley (Gloucestershire), England, who in 1796 performed the world’s first vaccination. Taking pus from a cowpox lesion on a milkmaid’s hand, Jenner inoculated an eight-year-old boy, James Phipps. …” …More
[2] Virology question of the week: What matters more, multiplicity of infection or virus concentration? - Virology Blog
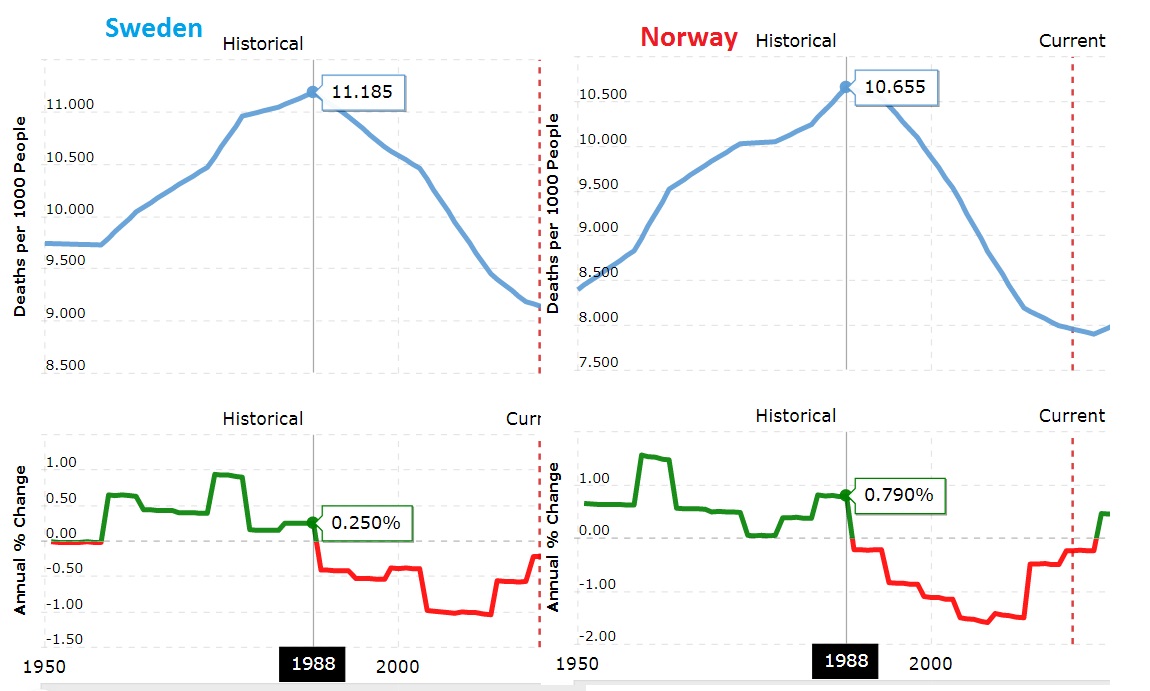
Sweden was indeed higher - for last year 0.92% versus 0.8% for Norway. Nothing to do with the current virus stuff, but both countries had a low rate (barely higher than for last year) after World War II, and then the rate rose to a peak in 1988, 1.12% for Sweden and 1.07% for Norway. After that a downtrend began. I’m wondering what caused that - WW II experiences that made for people dying earlier, 30-35 years later? Sudden Infant Death Syndrome peaked in Norway in 1988, but only provides a partial explanation.
The yearly death rate figures came from macrotrends .net and oddly enough they give a higher life expectancy for Sweden than for Norway, even while yearly mortality figures are the other way around. Worldometers has the same thing.
Is it as simple as people being afraid of others thinking they are “fat shaming” if they bring this up? I agree - there should be no hesitation to point it out.
This is a good question. In the U.S., it’s a considerable debate right now. Here in the state of Georgia, colleges were not going to generally require students to wear masks, but huge numbers of professors pushed back enough that now everybody’s going to be wearing masks.
For younger kids, my wife is a high school teacher, and to some extent there will be a choice - parents can choose to have their kids go to school or learn remotely, via computer, etc. - that is how the last school year ended and how summer school is proceeding.
Thus far, for the in-person stuff at school, teachers will be required to wear masks, but students will not. This is causing a fair amount of uproar, as in general it’s the teachers, not the kids, who will be most vulnerable to the virus. For older teachers and those with co-morbidity factors, many are saying, “No way…”
With so much of the U.S. currently having an explosion in virus cases and the death rates likely turning upward in the future, I doubt things are settled.
Quitting smoking? I think men are living longer longer now catching up with women… so may also be that the amount of physical work they do has decreased.
As for immunity… I think Belgium had one of the highest rates of spread but they are not finding much for immunity. Sweden I think is seeing the same. However, they had some researched published recently that said that T-cell production was up indicating that despite of what the antibody research is saying… immunity may still be stronger in Sweden than say Norway. Just no way to say for sure.
I think that most agree that economically Sweden will not be better off. They did cancel stuff there as well even if they did not have emergency conditions and total shutdowns but probably mostly because they are part of the general capitalist system suffering a bit right now.
Good questions. I was just struck by the similarity.
Belgium did indeed have a fast spread, and among countries of any size still has the highest per-capita death rate. But still a very low rate of positive tests, far less than 1%. Even allowing for some multiple of that with asymptomatic people who haven’t been tested, the population is still mostly vulnerable to infection, so those who are vulnerable should be taking serious precautions.
Doesn’t Sweden have lower death rates than the UK and Belgium (maybe it’s because a lower at risk population?).
I think we’ve all forgotten that the original goal was to flatten the curve, not eliminate the virus. Now we seem to be trying to eliminate the virus, which is a completely different thing.
Madeleine - I so totally agree that people have forgotten about flattening the curve and not overwhelming the hospitals so that they couldn’t cope and that now we seem to be trying to eliminate it. It’s not going to happen.
Sweden does have lower death rates than the UK and Belgium. People seem to continually compare countries that just aren’t alike at all. The UK has a more dense population that Sweden. We are all counting deaths differently too and probably adding in deaths that aren’t from Covid. The comparisons have all got a bit ridiculous in my opinion. Definitely not saying we shouldn’t proceed with caution but we have to start living again.
Saying the UK will suffer another 120000 deaths this winter is scaremongering from the journalists at their best.
I have been following the subject in many places (including official stats lists from various states) for some time now.
I find it interesting, as I get older, that there is this kind of holographic dynamic with our world. Not just metaphysically (that too, I’m kinda woo :-)) but in very real terms. I suppose because human nature is what it is, in every area.
It has reached the point where we do have numbers, but there are so many factors affecting them, and then more affecting who shares what and why and when, that it has become impossible to believe anything by anybody from any perspective. I feel this is the larger situation in our world right now as well, and a plethora of experts (who disagree not only with each other, but even themselves at different times!) combined with a lack of trust is having weird effects in the culture.
As an example of what I mean by numbers ‘affected’, here’s some:
First, what makes a ‘case’?
Official guidelines for hospitals, testing, etc., have made it clear that they do not need to test someone to report they are positive. There are a few ways this can play out, from merely assuming someone who died a month ago probably had it, to offering testing, and if one person in that masked, 6-feet-apart line of people tests positive, considering all of them positive since they were ‘at risk.’
There is a financial incentive to declare positives, and this is not just for any C19 treatment, but for ensuring that they actually get paid for someone who is dying of something else – hospitals very commonly do not get paid or all their pay especially for treatments followed by death.
The CDC officially states that a positive test for C19 antibodies doesn’t mean you have or had C19. There are other common viral experiences that will also show a positive result.
There is a very clear attempt on the part of organizations, as large as a state and as small as a single nursing home, to swing the numbers by force to whatever is best for them. It might be fewer deaths from it, to downplay that your governor just killed off a huge swath of the elderly by sending highly contagious people to your neither equipped nor trained for it rest home. It might be more deaths from it, to leverage requesting funding from all kinds of sources, all kinds of reasons. It might be making the number larger or smaller at political private ‘leaning’ on people because a Governor wants to re-open or a Governor does not want to re-open.
So as you see, we had already completely toasted even the method and the reporting for positive cases and this many months ago. It hasn’t improved much.
There is a nationwide issue with the way the stats are being run by the numbers per state vs. how the media is reporting them. In particular, just for example, sometimes “only positive test results are reported.” A ton of sources who are reporting testing results do this. This leads to a wildly skewed version of the % rate of affected citizens, which the news reports with great drama. But that statistic would be misleading because it is not based on all the tests. Many negatives are never reported. In some cases, they are reported, but not until later, when the stats for that source then levels out.
Now before anybody complains that it’s just numbers, consider that political policy, economic policy, health policy, and what may literally be the future not just of individuals over the next year+ but of a state and even a country, may be dramatically affected by such policies. Whatever they are going to be, they should not be based on manufactured, artificial, hyperbole-driven misinformation.
Continuing on prior bullet point: The reporting on numbers of cases and especially deaths is listed as daily but the counts are not solely from daily. You will see in the news, “OMG! State X had Z cases/deaths/whatever today! SO HIGH!” But when you look at the numbers, you see that in fact their ACTUAL number that day was quite low. The numbers reported officially to the state, however, were dramatically higher. Why? Because they have decided to “count” deaths that happened a week, a month, three months, ago in the official tally (hospital says, “Hey, we could count all these and government will pay us!”), and they have to put that number somewhere, and they can’t go back in time, so it gets added to today.
It is inaccurate to report these numbers on a daily basis “as if” they are daily totals when they are not, and it is a serious problem to form life-changing political decisions based on information like this.
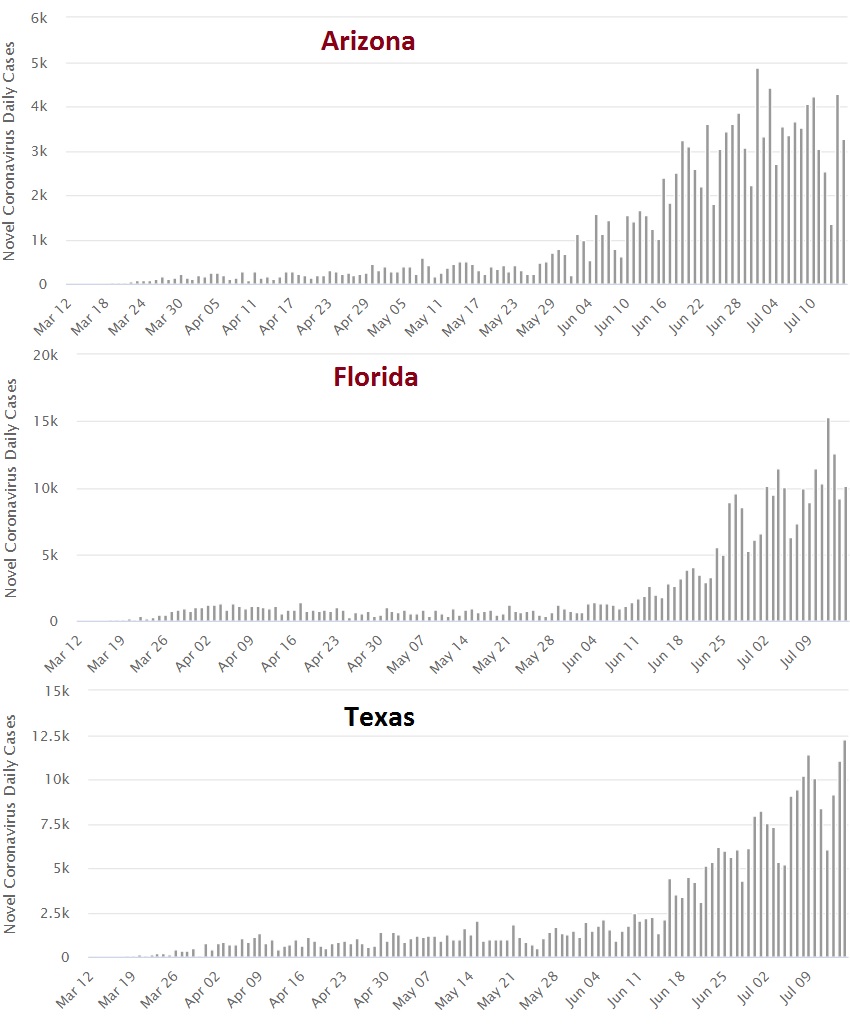
Just the other day in Florida, as an example of this issue: Orlando Health report: 98% positive rate. The hospital confirmed an ‘error’ in the report: the positivity rate was only 9.4%. Orlando Veteran’s Medical Center report: 76% positive rate. The center confirmed this was an error: the positivity rate was only 6%. This just goes on and on. Dozens of testing centers in Florida (or more) are reporting incredibly high rates – over 30 reported 100% recently – all of which are gigantic artifacts of them simply not reporting (sometimes until weeks/months later, sometimes never) the negative cases. Again, these numbers spawn media terror and political policies. This chronic inaccuracy is nearly as big a disaster for the people and the nation as the virus itself.
There is a fairly massive uptick in numbers in states bordering Mexico, and a wily evasion effort to either ignore or downplay this. Within those states at least in some like Arizona (AZ), the numbers are dramatically lower in most northern counties for example. Being a current intake port for a ton of people coming from a currently in super-high infection zone, is obviously going to affect their numbers in ways that have nothing to do with businesses reopening, for example. Failing to account for this is very inappropriate, especially when it concerns policy being set based on it.
The public is constantly bombarded with “comparisons” between countries, between states in the US. There is a dramatic difference in population numbers in these places. It is ridiculous to freak out about numbers twice as higher in state X than state Y, when maybe state X has 2-4x the population of state Y. Doing so is emotional misinformation. The only stats/graphs that have any worth in comparing (assuming we ignore all the points about the raw information to begin with, noted above) are those which are specifically how many cases and/or how many deaths vs. how many people in the population. For example, X# people died out of 100,000 population. Anything without that context is either useless or misleading.
Different states have had their ‘peak’ at different times. The testing quantity varies dramatically, which of course, will affect the number of positive cases found dramatically. New York around its peak was testing about 30-32K people per day. Florida has been testing sometimes 100K people per day. So the news drama about how Florida has more positive tests is just drama: of course they do.
The reporting on tests vs. the positive rate of the tests is regularly ignored by the media, in order to make things seem worse. For example, a few days ago (again in Florida which has been a big news focus lately) there was a big emphasis on how they had more positive tests that day, “a new record!” But in fact, the % positive on those tests actually fell to the lowest number in two weeks. (And that is despite all the only-reporting-positive-tests issues noted above!) So while in fact the stats and numbers were good news, the news media was reporting it as shocking and horrible news. They chose to ignore that of course more tests will find more cases, and chose to ignore that despite more tests, a smaller % of those people tested positive, in favor of what sounded dramatic (blood sells, as the old saying about newspapers goes :-)).
The devastation in the rest homes of five of the US states whose Governors demanded they take in contagious patients is a horrible tragedy, no doubt. But when we are counting deaths as a number (the ‘statistics’ of many, vs. the tragedy of those we love), presentations on numbers often ‘omit’ rather critical information that matters to the larger picture, that being: in a given period of time, how many people normally die? Yes, it’s going to be higher with a pandemic, no doubt. But looking at a raw number (let’s make one up: “10,000 dead!”) has a different impact on the already-traumatized public, than saying, “In this period, we lost 400 more people than we should have in place X, due to CV19.”
Somewhat related to the above point, using Texas as an example, they have a population of 29.68 million. In 2018, they lost barely under 12,000 people to the flu season. In 2019, they lost barely over 10,000 to the flu season. In 2020 for CV19, so far, they’ve lost just over 3,100 people. Yes, that’s tragic. But acting like this is the worst thing ever when in fact it’s (so far, we have until October to count) dramatically lower than the norm, is misinformation.
Of all our states, New York has a % of death so high it’s pretty much near the top of the world in stats – it doesn’t win because it’s part of the USA, and normally this is compared by country. Currently the news is attempting to make it seem like NY did really well and states like AZ, GA, TX and FL did horribly. This is an intentional narrative, not news. As of a few days ago when I was looking at this, NY had more than three times the death numbers (32K) as all four of those states combined (just over 12K) – while NY has only barely over 1/4 the population.
The current numbers of death (whatever accuracy current numbers have unless you can look at the sub-sub-details + read minds, see above) reflect a degree of herd immunity coming about. There are regions in NY where testing indicates as much as 68% of the population has been exposed – that’s huge! The number required depends, mind you, an 'estimate is 70%. Their current low numbers on deaths is in great part because the density of their population, and their severe exposure to the virus initially via inbound travelers from out of the country, basically killed off and infected so many people so fast, in some areas they have nearly arrived at HI at great speed.
Treatment: Hydrocholoroquine with an antibiotic + zinc is the standard treatment not only for C19 but similar illnesses (well before C19 existed) in tons of countries. Its primary value in this case is in preventing infection or in stopping it very early so it never develops into terrible symptoms. Of course that means you have to get it early – or at all. Politics caused it to be rejected in this country as the media took a case against it, and many governors banned doctors prescribing it. (And many doctors sued over a politician becoming a doctor by proxy and basically leading to terrible injury or death while the doctor could do nothing.) This has led to uncountable deaths, and uncountably more horrible effects that did not lead to death but are still horrible.
Despite many years of studies on this drug, and immense use of it, two recent studies came out the last several months saying it was not useful, which the media went forth with in a huge way. Only to discover that both of them (yes: both!) were basically data fraudulent, and after the fact the journals had to pull them. Of the literally endless number of ways this has all been politicized, few ways are worse than this – insulting and banning the only drug that is known to help save people, solely because the dude they don’t like in the Big Chair suggested it.
It is one of the most mass-used drugs in the world, for many decades now, and is incredibly cheap, I mean like less than two dollars a day. But if you prevent people getting it early when it can help them, and worse, if you nearly immediately intubate them as was done in NY (because they didn’t know better then), people are doomed. It’s a great help, but not much once you’re desperately bad off. This is still a struggle in many areas due to the mass mis- and dis-information about it.
Policy.
I think all of us saw the famous graph that supported “lockdown” that said the goal was to “flatten the curve.” The same number of people might die, but we wanted it to be more gradual so that our hospitals could cope. We did that. It’s done.
NY did not, partly because they didn’t have time of course, and that part is not their fault nor their leader’s, they were definitely at the front-end of the learning curve in the nation. (He has plenty of death he’s personally responsible for, but that front-of-the-curve factor is not his fault.) But the whole country shut down. We have done so much damage to so many areas of the country (and people, and businesses) that it will probably take 20 years just to fully recognize it all, and its forward effects.
The flattening of the curve, however, is done. Yes, we still have raises as other states finally start getting it in numbers, especially those bordering Mexico. But they are drastically smaller curves and they are nowhere near threatening the medical resources that were the entire point of the shutdowns.
No matter what drama you hear, the situation is not remotely as bad as it is being made to seem, and the arguments for new lockdowns are based on numbers that never in a million years would we have considered doing such a thing for six months ago.
Now it has somehow changed to eradication. This is absolute insanity, cannot and will not happen, not in our lifetimes. Anybody who thinks further lockdowns and that theory are reasonable should go watch the (surreal but prescient) movie BRAZIL a couple times.
It makes the high politicization of this topic – even more evident as what it is.
And I could go on (and on, and on) about that part, but I won’t.
I get the feeling of ‘throwing up our hands and screaming that none of it really matters,’ then. Overall, however, I think things are understandable and that the data has actually been fairly ‘smooth,’ country by country and region by region. I do think there are exceptions - China, Brazil, etc.
On the amount of cases, significant virus breakouts tend to make the total mortality substantially higher than normal. There are indeed many things pushing and pulling on the numbers, as you mention, but do you see anything that actually looks impossible or even truly surprising? We know that population density makes a huge difference, and that the virus breakouts are occurring at different times.
Currently, for the countries where most of the forum people are from, here are the reported infection rates:
1.1% U.S.
0.4% U.K.
0.3% Canada
0.04% Australia.
To me, these are low figures, indicative of being early in the virus outbreak, and not at all “obviously inflated.” Is there a rational argument that lower numbers are the true ones, versus the above?
For the U.S. states you mentioned:
2.2% New York
1.8% Arizona
1.4% Florida
1.2% Georgia
1.0% Texas
,
Same thing - low figures; it’s early. And it’s not like these are being falsely inflated to any significant degree. Even allowing for a meaningfully-large amount of people (compared to reported cases) who have been exposed, we still have a population where the vast majority have not been exposed, and this is borne out by the fast increases we’ve seen when the virus does get going, as in many U.S. states lately.
The state of Georgia does shift things around a little, i.e. a positive test result is first attributed to when symptoms were noted, or, next - to when the test was taken. Failing both of those, it goes on the date the test result was received. This makes it look like current case numbers are falling off a cliff, since many are not attributed until a couple weeks later. There is value to knowing when cases actually appeared, versus just when the result is reported, so I can’t argue too much.
In the end, all the numbers appear and things average out - there still is a ‘smoothness’ to the results, especially when the "weekend effect’ (lower reported numbers then) is accounted for. Week-over-week and month-over-month, nothing is much changed at all, by this method of reporting.
Here is what actually happened. The Florida Department of Health reported a 98% positive rate for Orlando Health. People naturally misconstrued this to mean the entire Orlando region, city, etc. The 98% figure came from the Orlando Health laboratory, where 512 of 522 tests were positive, which is indeed 98%.
There are many hospital labs in the Orlando area, and some had positive rates as low as 2%. The average was 10%, close to Florida’s overall rate of 11% positives among current tests.
Of course there will be mistakes, people messing up with a decimal point, being stupid, mathematically, failing to report cogently or interpret properly, perhaps even deliberately attempting to “massage” numbers in their favored direction. But overall such incidents are isolated and inconsequential, unless the perpetrators are high enough - so I’m talking about state level in the U.S. or higher.
I’ve seen no “terror,” and if ever there was a state that ignores the numbers, it’s Florida.
Who do you see actually “freaking out,” here? Hey, if somebody is saying that California is doing terrible because they have twice the number of cases as New Jersey, then that’d be a good example (and I’d argue with them as strongly as anybody). Yet I don’t see anybody doing that. We talk about per-capita this and that, and percentages. We compare a given state, country, etc., to the same entity in the past. Raw numbers are fine, too, though context certainly matters, as you said.
Have to disagree - it’s not “just drama.” FL’s death rate has turned up, and has been hitting new highs. There are twice as many people hospitalized for Covid-19 as when the restrictions were being lifted, i.e. bars, movie theaters, tattoo parlors, tanning or nail salons opening up, etc.
March - April - May, Florida really did keep a lid on things. But in June, with things opened up and a change in people’s behavior, it began to be a different world. Sure, there’s more testing now, but that’s far from the whole story. Again - overall Florida has had a 1.4% positive rate, and this was skewed toward the high side early on, due to mostly hospitalized and demonstrably sick people being tested. Now, the positive rate is 11% overall. And, 5 days ago Florida’s COVID-19 pediatric report showed 31% positives among those under 18 (16,797 of 54,022). It’s not like this is just coming from increased testing - this is a huge surge (and one that will actually result in some meaningful amounts of immunity, if immunity gain is as simple as we hope for).
That’s really not it. There were two faulty studies - no argument that they were messed up, stupid, illogical etc. - that can be disregarded. But there are many other studies, and results across many countries, that show that the chloroquine family is of little net benefit or is a net negative for Covid-19 cases. That is not to say that the medical science of treating the disease has not improved - it certainly has, to the extent that death rates are declining.
We now know that it’s not a “lung only” disease - many organs are frequently involved. We know that blod clotting is a major factor, all through the body (blood thinners like Heparin and Aspirin are making a big difference). We know that hypoxia kills a lot of the patients, even as they sometimes show no symptoms before things get critical (hypoxia actually usually makes one feel ‘happy’). We have the drugs Favipiravir and Remdesivir - these are proving to be effecive antivirals. We know that steroids can be used to prevent the cytokine storm (another big cause of death) in many patients. Oddly enough, it’s also been found that just lying on one’s stomach in the prone position helps with hypoxia. One very new thing is looking at the small blood clots that form in lung blood vessels - the gout drug Colchicine is showing some promise in preventing them.
If you get infected now, your odds are better than they were in Feb-March-April.
That’s true, but these are very small areas. There have also been groups of kids at summer camps and the like where most got infected. The 68% was in one clinic in one area of Queens, NYC. Such areas tend to be low-income and have much higher death rates, as well. Still, if immunity here “works” then some degree of ‘herd immunity’ should be present, there.
The worst hit area [zip code 11239 (13,000+ people)] of New York City has about triple the death rate of the city as a whole, ~0.66% versus ~0.22%.
Who is saying it’s the “worst thing ever”? And any place with a virus outbreak has a point where things are still small - it’s the nature of things. The virus has been in Texas for at least 5 months, and it was only a week ago that things really started to take off. We can pick similar points in time for NYC, etc.
It’s not done in most of the U.S. NY, NJ, CT, MA - okay, you’ve got a case, there. But look at most other states and it’s a different picture.
Seems to me it’s common to understate deaths from Covid-19 and drastically underemphasize the bad effects on those who don’t die from it. Most places where the virus has a substantial breakout end up with many deaths in excess of normal. Taking the reported Covid-19 deaths does not account for the ‘excess’ deaths. These remaining excess, not-currently-counted-as-Covid-19 deaths are 10,000+ in the U.K. (as of June 26), ~21,400 in the U.S. (June 6), ~17,200 in Mexico City (June 28), 16,300 in Italy (March-April), 17,000 in Spain (May 31), for example.
Of these deaths, some are indeed obviously not Covid-19. And some are, i.e. there’s an overall under-counting of Covid-19 deaths there.
For every death, there are several people who end up with permanent heart damage and/or lung damage. Those are the two biggest things. There are also greater numbers of strokes, neurological damage = loss of cognitive function, and neurological damage = loss of coordination/chronic weakness among the survivors, versus deaths. The number of people severely and badly impacted is a substantial multiple of the number of deaths. There is much more to come here - studies are only starting to come out. Last one I saw was in the Journal of the American Medical Association on July 10 - one study in Italy found 13% of people, 60 days after leaving the hospital, were free of bad symptoms and considered fully recovered.
It’s also common to overestimate the effect of government policies. Most of the effects on the economy here is due to people’s behavior changing, not what a gov’t does or does not do. One study (https ://voxeu.org/article/unemployment-effects-stay-home-orders) found that roughly 1/4 of increased unemployment was due to gov’t stay-at-home orders, with ~3/4 going to occur without such orders. People’s behavior change is the largest thing, and the markets knew that - they were plunging well ahead of gov’t policies coming out about staying home, etc. People quit flying, going to restaurants, movies, etc. - mostly not because the gov’t said so, but because the virus was a thing.
It’s really not done in most U.S. states. The first wave is only now really getting going. Being near Mexico or not, there are drastic increases in most U.S. states in June/July, whereas things were far quieter Feb. - May. Medical resources have already been stretched hard in many places. It’s happened already in Texas. Saw this today for Florida: 54 hospitals in the state now have zero available beds in their intensive care units and another 40 hospitals have less than 10 percent bed availability in their ICUs. https ://www.nbcnews.com/news/us-news/florida-hospitals-face-icu-bed-shortage-state-passes-300-000-n1233899?cid=sm_npd_nn_fb_ma&fbclid=IwAR0JgRzT87Tu_W2mXY6bsK9041yvLWYWHlCYcBqeGm5oiSdd4323j9fHY9o
Who do you see saying that? All along, have we not taken it for granted that, all other things being equal, most people will get exposed to the virus, eventually? The U.S. is still only reporting 1.1% of people as having tested positive. There is virus mitigation, and there is virus suppression - some countries have suppressed it so well that perhaps it is eradicated, there. Eventually, without sufficient hosts and transmission, viruses do die out. But that ship has sailed for the U.S.
If a vaccine is forthcoming, then what we are doing is bridging the gap in time to its arrival. We are also going from worse treatment to better treatment - it’s getting substantially better and perhaps will yet get massively better as we go forward in time, even without the appearance of a really good vaccine.
I can only conclude that the array of news I see – youtube, somewhat against my will, insists on showing me a few highlights from every channel in my lists of stuff to watch – is coming from Mars or something. That you see no media upset … and that you don’t even see that the ‘flatten the curve’ has shifted to something vastly more… we’re just not living in the same reality at all. I like yours better! I’ll leave you to it though. I took the time to write that post but I absolutely freaking hate this subject.
It didn’t take me long to realize that you can find support for any theory on the web and the over-abundance of just plain bullshit that is being spewed is exhausting if you try to weed through it.
YouTube – well, that at least partially explains things. But how about one link or example of what you mean?
I really don’t see “media upset.” Sure, TV news, for example, tries to make things sensational - “if it bleeds, it leads,” etc. And Florida, Texas, Arizona, etc., have recently been in the news. But things really are (finally) changing fast there. I think this is entirely consistent with reality and furthermore - that it was entirely predictable and to be expected. When you have the overwhelming vast majority of a population as yet uninfected, what is going to happen when the virus does start really breaking out?
Things were pretty quiet for a long time, and then WHAMMO they changed. This is just fact. And what rational reason is there to think that it would not happen?
I’m not sure what you mean here. I’ve said for a long time that most U.S. states have a population that was very vulnerable because they had no significant exposure yet. Some relatively few states have had big ups and then downs - while they definitely flattened the curve from what it would have been had nobody done anything, in no way did they really keep things “flat” (like some other countries have done).
For the rest of the states, things were “flat” but that’s because the 'first wave" had not really gotten started yet. Now we see it in a lot of states.
All the decent evidence is that it’s being undercounted, actually, often due to political pressure.
Ah yes, if you disagree, it’s always the media beating things up. Things aren’t actually bad, and other countries that weren’t idiots aren’t actually doing much better, it’s all just pretend.
Very patient and well put together response that will no doubt be ignored because it doesn’t fit the “everything is just made-up drama” mindset. How anyone can look at those graphs and blame it on the media getting excited is amazing.
Yes actually I do disagree. My prerogative. The media don’t actually always help themselves. Early on we had pictures of Brighton beach. It was rammed. People weren’t allowed out at the time. Everyone was disgusted at the way people had behaved. Well guess what? The photo wasn’t even taken this year and all I said was that it was scaremongering. I did NOT say that things weren’t bad. I did NOT say that other countries weren’t idiots and were doing much better. And I did NOT say it was all just pretend. Please don’t twist an innocent comment into a tirade.
The 120000 is scaremongering. The report in reuters said it was worse case scenario, covers 9 months and is only a possibility if absolutely nothing is done. Yet the report the vast majority of the population get is just that we could suffer 120000 deaths this winter. That is putting things way out of proportion
And whether you like it or not, different countries are counting deaths and cases differently, even within the uk.
And as it just so happens I personally am taking all this stuff very seriously and treating it with a healthy respect that I think it deserves.


 Great phrase.
Great phrase.
 But how about one link or example of what you mean?
But how about one link or example of what you mean?