
Hi,
Let me start first with I thought I was going to have to find a new doc. When I told her via email that I started the ketogenic diet, her response to me was “I can tell you that I will not support a diet high in fat”. And I reminded her of that comment today when I saw her. She was surprised and asked how long ago that was, and apparently since then she has attended a conference on obesity and she is much more educated on this WOE.
I don’t have the lab results handy, but my total cholesterol is higher–260 now where it was just under 200 previously. LDLs higher–she seemed worried about this. Triglycerides significantly lower. HDLs almost doubled. Where as previously she was almost refusing to run more tests on my LDLs, now she is fine with it but I couldn’t remember the name of the test. Can you tell me the name of the test that it is called in the US?
Also, she said that she learned in her conference that the lipids results go up, but then come back down. She thought they should be coming down about now. I have been on this WOE for 6 months. Any information on this?
Also, my cbc, cmp, and hgb A1C all normal. She was pretty stoked about the LFTs being normal. Also she has suggested I return in 6 months and wants me to check a body fat composition–especially for visceral fat. Since my LFTs were normal, not sure why, but sure, why not.
Thanks in advance.
First labs since starting keto
From what I have learned, and there are much smarter people in here, total chol. number is useless. For a standard lipid test, the trig/HDL ratio is the main indicator. So unless you can get the particle count test, I would focus on that ratio <2.0 is considered good.
This is significant. Well done. And it is very encouraging to hear of a doc who has educated herself on the current nutritional research.
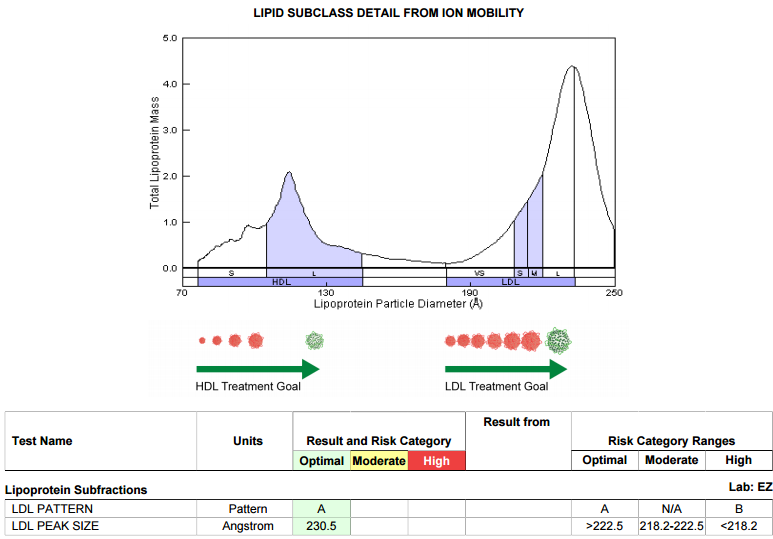
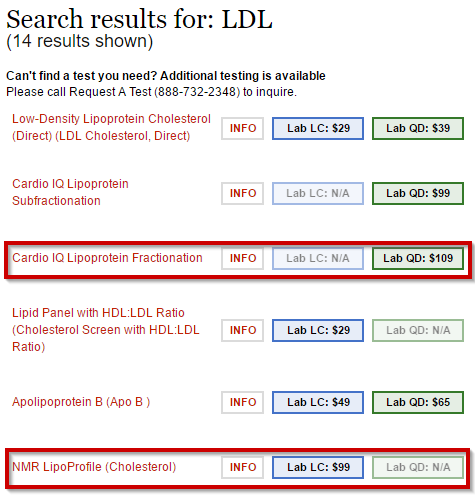
Through Quest Diagnostics it is known as the “Cardio IQ” and provides the lipoprotein subfractions with a portion of my actual results shown below.
I believe Lab Corp calls it the “NMR LipoProfile” for Lipoprotein Profile.
For reference, both versions are available from Request A Test
http://requestatest.com/tests/search
I just got the results of the Lipoprotein fractionization test and it’s great news! The majority of my LDLs are NOT the small density LDLs. I’m thrilled.
I remember the relief I had the first time I received confirmation that I was not at increased risk from LDL, what a thrill. 
See also:
For another relatively quick fix (prior to doctor-led tests when you just want to get the numbers down because you know they worry about them even if you don’t) there is also:
niacin (not nicotinamide) and vitamin C (l-ascorbic acid).
If you’re taking the flushing niacin (which is best really, if you can stand the flush) be careful to build up to it slowly in 10s of mg doses, getting slowly up to about 3g/day.
cf. “Niacin: The Real Story” by Hoffer, Saul and Foster.
(I think Hoffer believed that niacin (which is pretty important in the body and has a lot of functions, like vitamin C) helped to heal damage to the endothilium of the blood vessels. Vitamin C also helps. Thus this combination of vitamins was actually helping to get to the root causes (well, the immediate root causes) of the problem, and not purely fixing the symptoms (in the way a statin does).
Interesting article reviewing the studies done on niacin. http://www.docsopinion.com/2017/01/09/niacin/
Thanks for that link @chan_cleland. I’d read that as broadly positive for niacin, although they claim that clinical outcomes were not improved.
I wish they wouldn’t refer to it as a “drug” (when it’s a natural substance), and I wish they hadn’t tried to shoehorn it into statin therapy, although I suppose that’s inevitable now.
In my experience, the problems with flushing are exaggerated, although Hoffer did admit that some people could not tolerate it at all. He preferred it because of the blood lipid properties, and he preferred the instant action version over delayed-release versions because it was the latter than seemed to have the most side effects (other than flushing).
If you build up to it slowly, and then take it every day, the flushing eventually just does not happen. However, if you stop taking it for a few months and then restart, then the flushing will probably return, and you have to get used to it again. Once I had got used to it, I found it no problem whatsoever. I used to take 3g daily or more, together with vitamin C in fairly large doses (more than the 1g that is mentioned in one of the studies in that link).
Something else of potential interest is the so-called “Pauling Therapy” for CVD, which is basically vitamin C to bowel tolerance, l-lysine, l-proline, vitamin D, vitamin K2, various other vitamins and minerals, and some people would add niacin. There’s a lot of info about this on the Vitamin C Foundation website.
Now Pauling wasn’t a low-carber, although he did advocate minimising sugar, so I would think that most tests of the PT (and of niacin for that matter) have taken place against a background of the standard American (or western industrialised) diet. Personally, I think the PT (plus niacin) plus low-carb/keto diet would offer the best hope of heart health. (Although I’m aware that it is believed that a low-carb diet reduces the body’s need for vitamin C, so on low-carb keto, the doses that Pauling recommended may not be necessary (although it might be advisable for people in the early stages of keto to take at least some vitamin C, because they are still in a potentially long healing process, and there is no known toxic does of l-ascorbic acid, so even if you are taking more than you need, you aren’t doing any harm. Yes, you may be peeing expensive urine, but as Pauling said, it’s not such a bad thing for the urinary tract to get regular doses of something which will keep infections at bay. Similarly for the GI tract if it should cause loose bowels.