His concern is that our butyrate-producing bacteria are not encouraged on a ketogenic diet and he says he sees lot of people clinically that have low counts of butyrate-producing bacteria. This, he puts it down to lack of consumption of legumes (i.e. chickpeas) once a person has gone past an initial resetting of the hyper immune responses.
His second claim was that a long-term KD can lead to total extinction of certain bacteria populations. I believe this claim is dubious and needs solid research to back it up. He claims to have seen it clinically it seems.
I just dug out one study on the matter. Here is an excerpt:
" Analysis of butyrate production potential
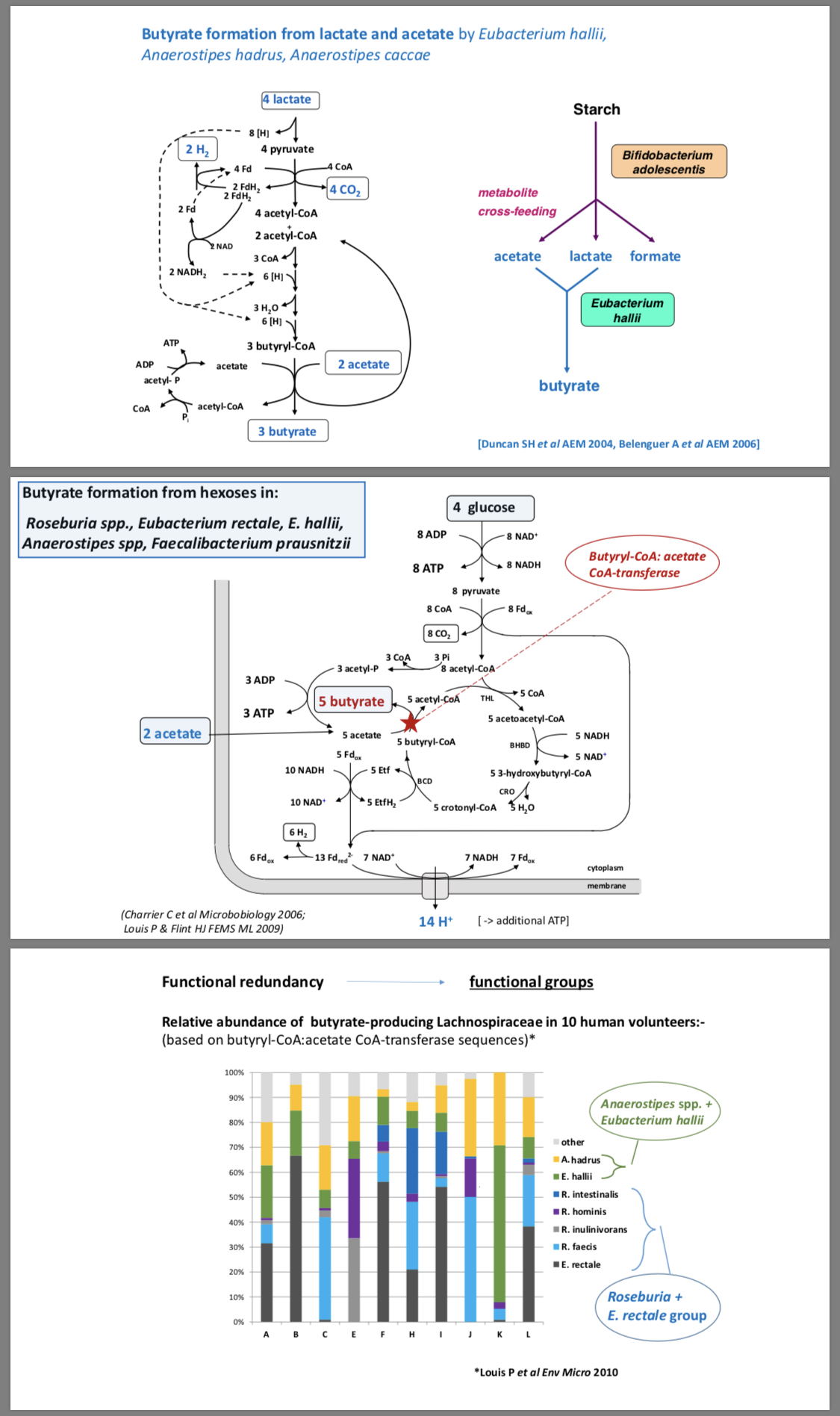
E. rectale , a major butyrate-producing species in the human gut, significantly decreased proportionally in patients during KD. To analyze whether this might impact the total butyrate synthesis potential of the whole community, a bacterial butyrate synthesis gene database20 was used to identify reads from genes involved in butyrate production in our shotgun metagenomic dataset. RPKM (reads per kilo base per million) values were calculated for all genes of the known microbial butyrate production pathways upstream of bcd / etfAB (butanoyl-CoA dehydrogenase, E.C.: 1.3.1.109), as there are downstream overlaps between pathways. gcdB of the glutarate pathway was excluded owing to recruitment of many false positives.21 Four butyrate-producing pathways are currently identified in human gut microbial communities20; the acetyl-CoA, the glutarate, the 4-aminobutyrate, and the lysine pathway. KD intervention did not have any overall significant impact on the relative abundance of any of these pathways (Fig. 5 a, band Fig. Supplementary Figure 2 a, b). Interestingly though, we found that genes from the most abundant butyrate-producing pathway in the healthy human gut microbiome, the acetyl-CoA pathway, were less abundant in our patients compared to controls already before starting KD. Here a very weak but inverse correlation was detected between age of the patients and relative gene abundance indicating that the lower relative abundance of genes of the acetyl-CoA pathway in our patients (Fig. (Fig.5c)5c) compared to our controls before KD was not due to the age difference between both groups. Rather, increasing age in our patients might increase the difference to the controls. An opposite trend was shown for the 4-aminobutyrate pathway (Fig. (Fig.5d).5d). This pathway was shown to be less relative abundant in the healthy gut microbiome compared to the acetyl-CoA pathway.20 In our cohort, genes of this pathway were more frequently identified in patients compared to controls before KD and a possible, yet not significant, further proportional increase was experienced during KD. Relative gene abundance seemed to slightly increase with age of the patients, indicating that this observation cannot be explained by age differences in the patient and control groups either. The lysine pathway did not show any significant differences in relative gene abundances within or between the groups at either time point (Supplementary Figure 2a). In the glutarate pathway, the relative abundance of one out of the six genes ( hgCoAdA ) was significantly decreased in the patients (Supplementary Figure 2b). However, the relative abundance of the concomitant enzymatic subunits hgCoAdB and hgCoAdC or other genes involved in this pathway was not decreased. It therefore seems unlikely that the glutarate pathway relative abundance is significantly different in any group of samples.
Analysis of butyrate production potential. RPKM (reads per kilo base per million) values for unique genes of the acetyl-CoA pathway a and the 4-aminobutyrate pathway b for butyrate production. Data are presented as follows: center line, median; box limits, upper and lower quartiles; whiskers, 1.5× interquartile range; points, outliers. Dunn’s test of multiple comparisons with Benjamini–Hochberg adjustment: * p < 0.05, **p < 0.01. Ctrl control, Pat patient. White, Controls time point 1; Ivory, Controls time point 2; Green, Patients time point 1; Red, Patients time point 2. Correlation of RPKM of each gene to age of patients at time point 1 for the acetyl-CoA pathway c and the 4-aminobutyrate pathway d . None of the correlations were significant ( p > 0.05). thl acetyl-CoA acetyltransferase (thiolase), bhbd β-hydroxybutyryl-CoA dehydrogenase, cro crotonase, abfH 4-hydroxybutyrate dehydrogenase, 4hbt butyryl-CoA:4-hydroxybutyrate CoA transferase, abfD 4-hydroxybutyryl-CoA dehydratase and vinylacetyl-CoA 3,2-isomerase (same gene)"
That’s far too scientifically dense for me but I think it is saying that the possibility for extinction of certain bacterial species doesn’t actually exist, as the pathway is maintained throughout Keto and the bacteria will consume acetate compounds.
Then there is the following excerpt:
" The relative abundance of the genus Bifidobacterium was significantly decreased in patients after 3 months on KD. The species B. longum and B. adolescentis were significantly reduced but a similar trend was also observed for other bifidobacteria such as B. bifidum and B. catenulatum (data not shown).
Bifidobacteria are common to the healthy human gastrointestinal tract. They metabolize complex carbohydrates and possess one of the largest predicted glycobiomes25 including genes encoding for a specific hexose fermentation pathway called fructose-6-phosphate shunt or “bifid” shunt.26 This pathway is superior in the energy output produced to pathways used by other fermentative gut bacteria and provides a growth advantage for bifidobacteria in the presence of complex carbohydrates. These facts may explain the concomitant proportional decrease of bifidobacteria and genes involved in carbohydrate metabolism during KD.
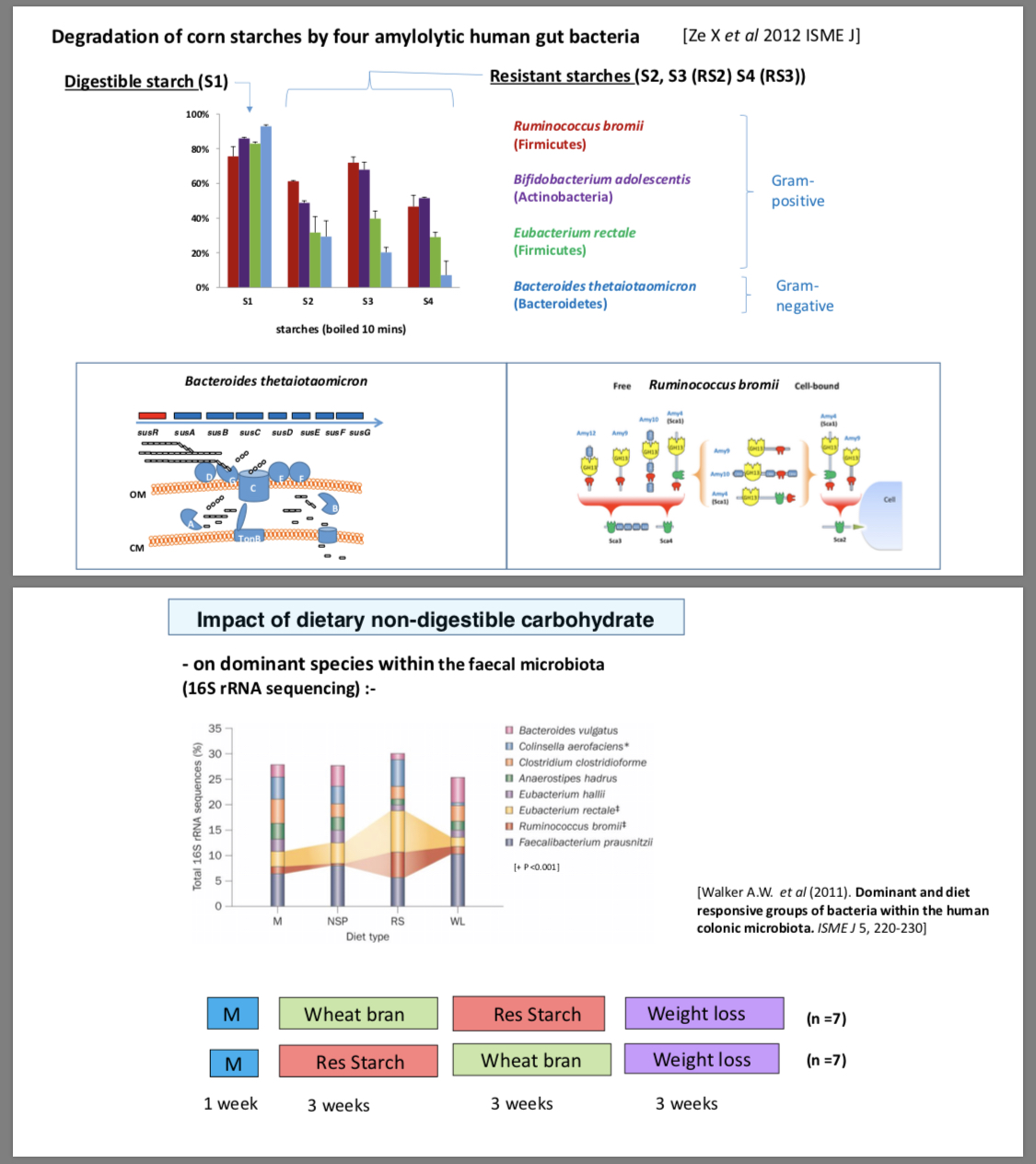
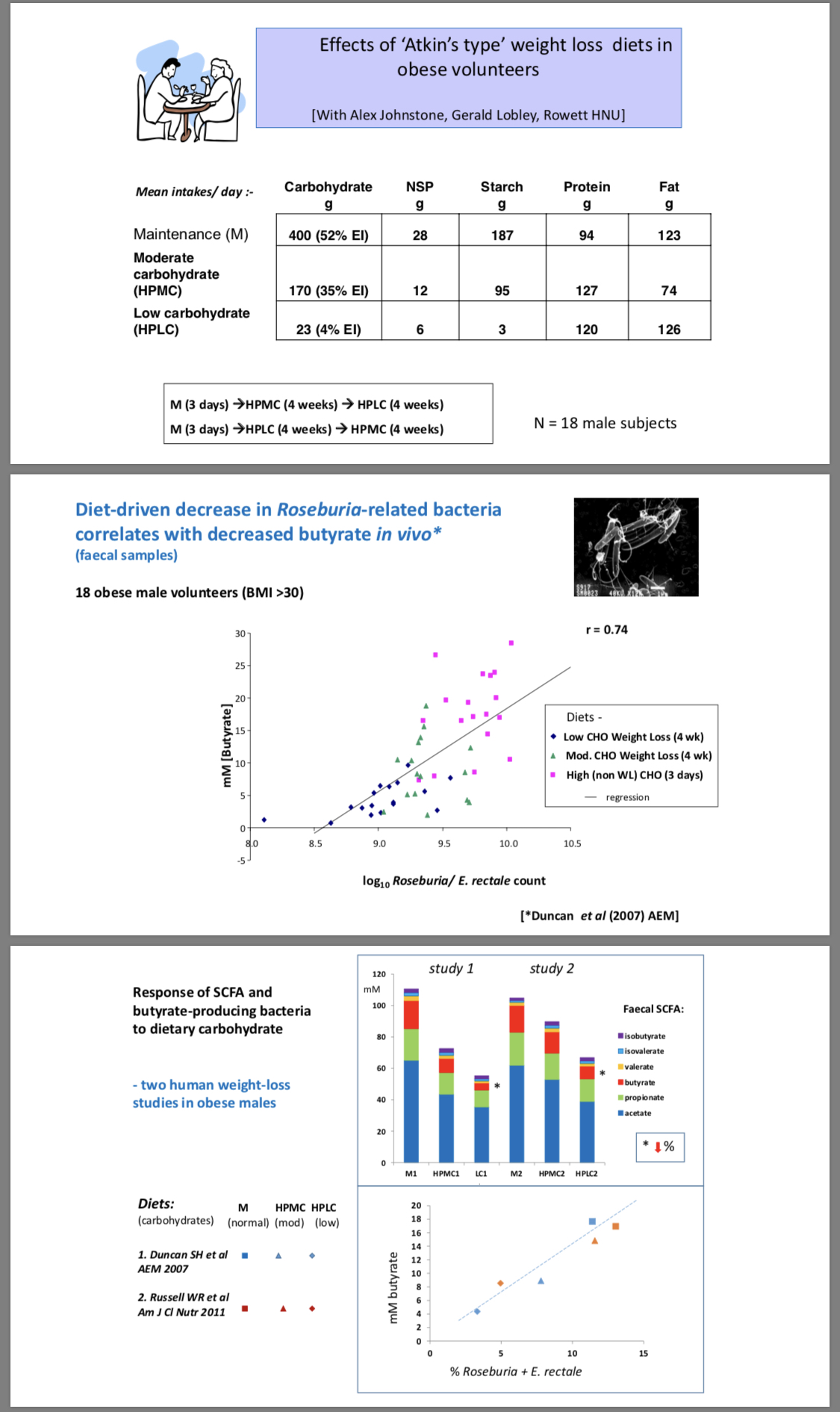
Duncan et al.27 supports our findings of diminished relative abundance of bifidobacteria and E. rectale in a low carbohydrate diet as well as our hypothesis that this may result in lower production of acetate and lactate. Acetate and lactate are products of the bifid shunt. Both acids contribute to a decreased pH in the gut, which may prevent pathogen growth. More specifically, Fukuda et al. has shown that bifidobacteria can protect mice from infection by enteropathogenic E. coli O157:H7 through production of acetate.28 In our study, we show that bifidobacteria relative abundance decreases during KD and E. coli relative abundance increases. This may, at least partly, be due to a decreased acetate production by Bifidobacterium and/or an increased luminal pH. Agus et al. demonstrated that a Western diet rich in both high fat and high sugar increased the relative abundance of Proteobacteria in mice that correlated with intestinal inflammation and increased susceptibility to adherent-invasive E. coli infection.29 E. coli is a versatile species comprising both commensal and pathogenic strains and can consume carbohydrates from a variety of sources through cross-feeding, including dietary fiber but also shed epithelial cells, and mucosal polysaccharides degraded by intestinal anaerobes.30 E. coli is associated with a variety of chronic intestinal diseases, including inflammatory bowel disease (IBD).31 Therefore, the expansion of E. coli during KD might be of concern for general gut health in our patients.
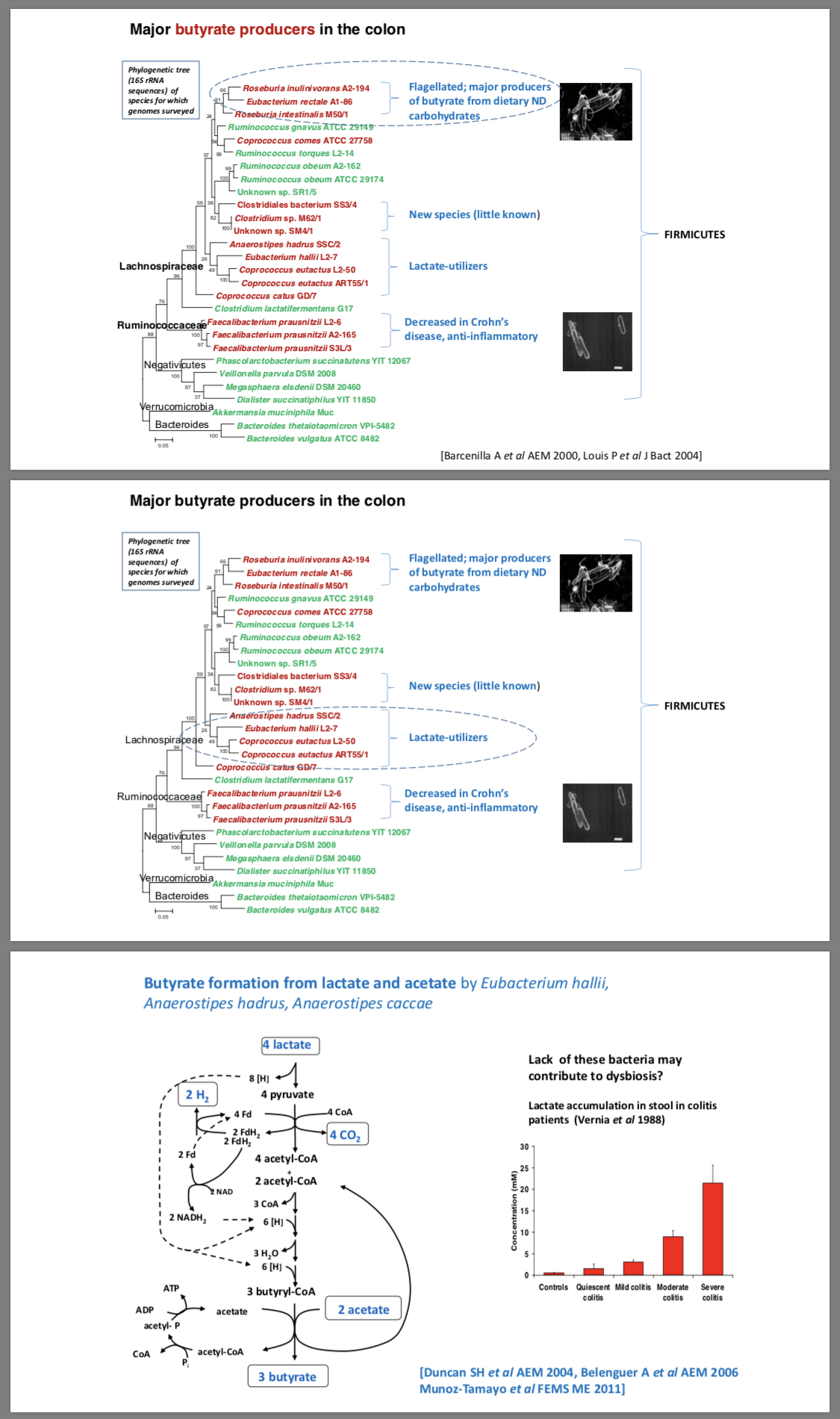
Acetate can be consumed by butyrate-producing gut bacteria. Riviére et al.32demonstrated mutual cross-feeding between B. longum and E. rectale . This may contribute to the concomitant decrease of E. rectale relative abundance in our dataset. The reduced consumption of certain carbohydrates (resistant starch or wheat bran) may also have had a direct effect on the proportional decrease of E. rectale .33,34 A consequence of the depletion of Bifidobacterium and E. rectale may be a decreased production of short chain fatty acids (SCFA), specifically acetate in the bifid shunt and butyrate by E. rectale . SCFA are important for overall health and low fecal amounts have been associated with diseases such as IBD35 and advanced colorectal adenoma.36 Both acetate and butyrate have been shown to have anti-inflammatory activity.37–42 In addition, butyrate has a direct effect on gut health, being an essential energy source for colonocytes and increasing the intestinal barrier function.43,44 In our dataset, the relative abundance of E. rectale was rather low in the patients before starting the diet but further decreased during KD. However, the butyrate-producing community is a taxonomically diverse functional group.20"
…
That excerpt highlights the “lowness” of the butyrate producing bacteria and the “highness” of e.coli. But it doesn’t anywhere that I can see imply the “extinction” that Dr. Hawrelak claims. There appears to be no mechanism for extinction because the bacteria is at least getting some of its needs.
Overall, I’m not sure why he’s so anti-keto as my reading of the research is that we want to make sure we get adequate NDCs (non-digestible carbohydrates) which essentially have zero insulin/glucose response and will directly feed the key gut bacteria (bifidobacteria and butyrate-producing colon bacteria).
" There are two ways to get more of the fatty acid butyrate into your diet. The first way is to directly consume it. The name butyrate comes from the Greek word “butter.” Butyrate is found in butter and other forms of diary—especially goat, sheep, and buffalo milk."
So his claim that a KD risks extinction of butyrate producing bacteria is sounding more and more far-fetched to me. Am I missing something?
Dr Hawrelak’s final recommendation was to consume a wide diversity of NDC (non-digestible carbohydrate) fibre. Which he equated with legumes and fruits (along with vegetables that of course many ketoers already consume).
It seems to me that it would be helpful to differentiate different versions of a Keto diet in research studies and claims about KD. It doesn’t seem good enough to say “I saw a keto person and they were unwell.”
I know, for example, that my keto diet is wildly different to other peoples. For example, I never eat bacon and I consume loads of micro greens and sprouts and a range of different NDC vegetables. I even consume sprouted mung beans and lots of berries so I’d be curious how my gut would compare to his usual KD patients with gut issues.
I do think the issue is far more with long term induction-phase-only (0-20 grams carbs) keto that certain kinds of non-IR folks do to optimize performance goals (often high protein, moderate fat, and nearly zero carb for 6-7 years) as opposed to a well-formulated ketogenic way of living which is different - a la Westman, Phinney & Volek, and Dr. Atkins Phase 2 and Maintenance, and the Drs. Eades Phase 2 and Maintenance. None of these ketogenic physicians prescribed induction phase keto as a longterm way of life - the whole idea was phases, metabolic healing, and a sustainable food culture.
A key factor is that the foundation microbiome in many folks in industrial society is a gut that was populated by SAD balances of bacteria from infancy. Those of us born and raised in industrial society don’t have Inuit or Masai microbiomes, we often have hugely imbalanced microbial populuations. Many of us were fed formula/corn syrup as infants/toddlers, and that has had an impact on our guts. Also, those born surgically without microbial maternal transmission have had additional microbiome challenges from the get-go. Then there’s overuse of aggressive antibiotics in childhood and adulthood! It seems everyone in the high carb industrial foods world has gut issues of some kind, and a well-formulated keto lifestyle heals through gut transformation and adaptation to calibrated increases of veg fiber or resistant starch.
Some resources I’ve explored are Dr. Grace Liu, a pharmacologist, who has worked with a number long term carnivore ketoers (as in 6+ years of extremely LC for performance/athletic purposes) in restoring their microbiome. She also recommends soil-based organisms for severe cases. Her program is about building “a warrior gut” via some amount of fiber/resistant starch.
Microbiologist Norm Robillard PhD (author of Fast Tract Digestion) specializes in reducing gut fermentation and renewing good bacteria populations with minimal and specific kinds of veg/fruit fibers. His approach is a different routine - because folks with excess gut fermentation need to calm the gas production and stop the bacterial overgrowth in the small intestine.
If the good bacteria in the large intestine are capable of producing huge amounts of butyrate (far more than one takes in from butter) - I like the idea of keeping them well fed. And they eat fiber. So I try to eat various resistant starches/fibers throughout the week, in small portions. Some days I have an apple, other days, a couple tablespoons of ghee-fried chilled & fried white basmati rice. I also try to take at least one tblsp of coconut oil per day - which is amazing for boosting ketones/BDNF. Brain maintenance is a daily practice!
”…Hmm, I wonder where the name BUTYR-ate came from? Butter perhaps?[2]…”
Organic Grass Fed Butter (the only kind of butter I will eat) is full of butyrate but I also include Type 2 resistant starch in my diet which may be an occasional green banana or raw sweet potato sticks (I keep in the fridge in a glass of water) to keep mucosal barriers and tear production up to par (dry eyes on keto) and also to feed those gut bugs (“butyrate producing bacteria?”).
This so called “missing butyrate” and if that “butyrate producing bacteria” is really a thing or need for concern then I see no problem as to why it would be a problem on a well formulated Ketogenic diet?
Where do these numb skull critics (doctors) get this stuff?
Notes:
[1] “…Here’s where the fun stuff happens — resistant starch acts more like a prebiotic than a typical starch.[2] A prebiotic is what your good gut bacteria (probiotics) eat. So once the resistant starch arrives in the colon, your good bacteria feeds on the starch, producing something called butyrate (butyric acid).[3] Butyrate is a short-chain fatty acid that strengthens your brain and your gut.[4][5] Grass-fed butter is high in butyrate — one reason why it’s such an important element in the Bulletproof Diet. …” …More
[2] ”…Finally, as pointed out at the WholeHealthSource website, “Butyrate Suppresses Inflammation in the Gut and Other Tissues”: “…There are two main ways to get butyrate and other short-chain fatty acids. The first is to eat fiber and let your intestinal bacteria do the rest. Whole plant foods such as sweet potatoes, properly prepared whole grains, beans, vegetables, fruit and nuts are good sources of fiber. Refined foods such as white flour, white rice and sugar are very low in fiber. Clinical trials have shown that increasing dietary fiber increases butyrate production, and decreasing fiber decreases it. Butyrate also occurs in significant amounts in food. What foods contain butyrate? Hmm, I wonder where the name BUTYR-ate came from? Butter perhaps?” So yes, although you can overdo butter just like you can overdo coconut and MCT oil, if you are indeed consuming lots of LCFAs and MCTs, consume a bit of butter too. Thank you, Dave Asprey and Bulletproof Coffee, for pointing that out quite extensively. …” …More
Hmmm, my nutritionist (my PCP’s husband actually) told me to eat cooked and refrigerated white rice every day. I haven’t been doing it because I was afraid of the carbs. This article says exactly the same thing he told me. Guess I’ll have to try it again.
The resistant starch in cold rice is only a fraction of the starch, not all of it. Successive heatings and coolings will increase the amount, but there will still be regular starch.
Ketones in the blood perform a similar function with regards to colonic cell as butyrate in the digestive tract.
Also, check out this topic:
PaulL
(You've tried everything else; why not try bacon?)
#11
This is a bogus concern, since any dietary change affects the gut biome. Prof. Bikman even jokes, in one interview I saw, that fasting is a great way to kill off all your gut flora and fauna, and start fresh.
Furthermore, β-hydroxybutyrate is just as good for colon cells as butyrate, and helps tighten up the gaps that cause IBS just as well. So why worry about lack of butyrate, when you’ve got plenty of β-hydroxybutyrate to fill the need?
Thanks everyone for your replies. I’m leaning towards this doctor having a bias against keto. I guess he sees people on unbalanced keto diets who have come from unbalanced SAD diets.
I might contact him and ask him if we has some research to back up his claim about the extinction of certain good bacteria. That was his strongest claim (around the 50min mark).
He claims he gets it from patients who come to him on the keto diet and have inflammation issues. He tests their bacteria colonies and it comes up with lack of diversity and extreme lows on butyrate producing bacteria. In fairness, the research I posted showed a similar outcome.
The real problem I see is that these doctors are not taking care to note (as you say) whether it is a well-formulated KD.
I believe it’s fair based on our experiences as ketoers to assume it isn’t well-formulated diets… but it would be nice to confirm this.
Ketogenic is a macronutrient guideline, not a strict menu. People misconstrue that to mean any fat is okay and any protein. You can chug vegetable oil and eat soybeans to satisfy the ketogenic macros.
Quite different from eating animal flesh and fats.
So, you don’t feed your gut a lot of fiber, you will likely starve the fiber digesting bacteria. The fiber digesting bacteria is what produces butyrate in your gut, so there’s that.
But, if you’re eating sufficient butyrate (aka SCFA), you don’t need to make your own from fiber fermentation (and release the gas… https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5390821/ ***). Your gut bacteria is cool, in that it will adapt to what you’re doing. If you are ingesting sufficient SCFA, it will not need to ferment them, and yes, you might have some die off. So what? You’re not eating a bunch of chickpeas, so why do you need them? And if you want to eat a bunch of chickpeas, guess what… you’ll reestablish the colony in reasonably short order.
This is a bunch of scare. That said, I regularly consume a serving of black beans, more because I like them, than for any supposed butyrate benefit. Send me to Keto Jail, because I consumed a legume… /s
***The microbial conversion of complex polysaccharides to monosaccharides involves various biochemical pathways, which are mediated by the enzymatic activities of microbes. The main bacterial fermentative end products of complex carbohydrates are SCFAs, namely acetate, propionate, and butyrate, and gases (H2, and CO2).