
I never checked my bg before except for yearly blood work with my doc. It was always around 110. It’s still at least that high in the morning and I started keto in Oct 2017. About 3 months in I had a fasting insulin of 10. I’m 56 now so I’m wondering how much can I actually repair my metabolism at this point. I work from home but my job is stressful so that throws dirt on my trail as well.
Does a healthy ketogenic diet cause irreversible insulin resistance?
SunnyNC
(SunnyNC)
#78
Fry, I enjoyed reading all your responses. Any new updates? I am replying just to keep this awesome discission going. I am still not understanding why it’s ok to have higher fasting BG while on keto … high BG is high BG, regardless of the reason and we know high BG is not good. Saying your BG is high because your insulin is low on keto makes it sound like T1D (just for analogy purpose, I know T1D is a million times worse).
SunnyNC
(SunnyNC)
#79
Awesome discussion. Any new updates or a new thread with latest discussion? I am replying just to keep this awesome discission going. I am still not understanding why it’s ok to have higher fasting BG while on keto … high BG is high BG, regardless of the reason and we know high BG is not good. Saying your BG is high because your insulin is low on keto makes it sound like T1D (just for analogy purpose, I know T1D is a million times worse). If anyone has found any new studies that answers this iam interested. Thanks!
PaulL
(You've tried everything else; why not try bacon?)
#80
It’s all relative, but the simple explanation has to do with glucose sparing by the muscles, once they are fat-adapted. Serum glucose is tightly regulated, if we are not jacking up the level with an excessive carb intake. It naturally rises and falls throughout the day, but should stay within a fairly narrow range. Dr. Paul Mason, the Australian sports physician, says that he’d rather see stable levels in his patients, even if they are what some would consider high, than wild fluctuations.
As for “adaptative glucose sparing,” also called “physiological insulin resistance,” here is an explanation:
SomeGuy
(Joey)
#81
Fascinating. Not sure I fully grasp every nuance, but the different needs of muscle vs brain tissue for glucose provides an “a-ha” moment for me.
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#82
My understanding is that the brain given ketones as an option will select the ketones for fuel even when it has glucose as an option. In other words, when available, ketones are the preferred energy option. When you see the differences between ketone and glucose metabolism you understand why this is probably so. Ketones yield more energy per unit and produce less waste to deal with. I may have got this from one or several of Bikman’s talks, but can’t cite anything at the moment.
I interpret the brain’s ketone preference to mean that given sufficient time to adapt and sufficient ketones, the brain’s demand/need for glucose will gradually decline. There’s some debate about just how much of the brain’s energy requirement can be met by ketones - some think it maxes out at about 2/3 to 3/4; this is the current paradigm. Bikman thinks ketones could satisfy 100% with full adaptation and sufficient ketone availability. Whatever the ultimate total of energy supplied by ketones, as the brain uses more ketones for energy gluconeogenesis should scale down, since the brain has the biggest demand for glucose and if it’s demand decreases then the synthesis of glucose should follow.
I note that in the article cited by @PaulL , Peter says “I spend rather a lot of my life in mild ketosis” and I suspect that the fasting blood glucose rise noticed by Peter and others might in fact be due to having insufficient ketones available for the brain to max out, so it’s demand for glucose remains. As long as the brain says “feed me!” gluconeogenesis is there to do just that. When the brain stops asking for more glucose, I think gluconeogenesis stops making so much.
This would help explain why exogenous ketones have been observed to lessen the symptoms of brain disfunction among older folks who are still eating SAD. If indeed the brain prefers ketones it’s not going to be particularly fussy about whether you ate them or synthesized them in the liver. All that matters is they’re available and it uses as much as it can.
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#83
I have to go to work, so I don’t have time at the moment to comment. But I also think this might have significant bearing on another ‘mystery’ for those of us who have been keto for several years and experience a marked reduction in measurable ketones. More later!
PS (Next day!) Finally getting time to follow up. See following posts.
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#84
Comments in following post. I will there draw attention to items in the diagram and quote portions of the paper. I’m posting the diagram and the paper here separately for easier reference.
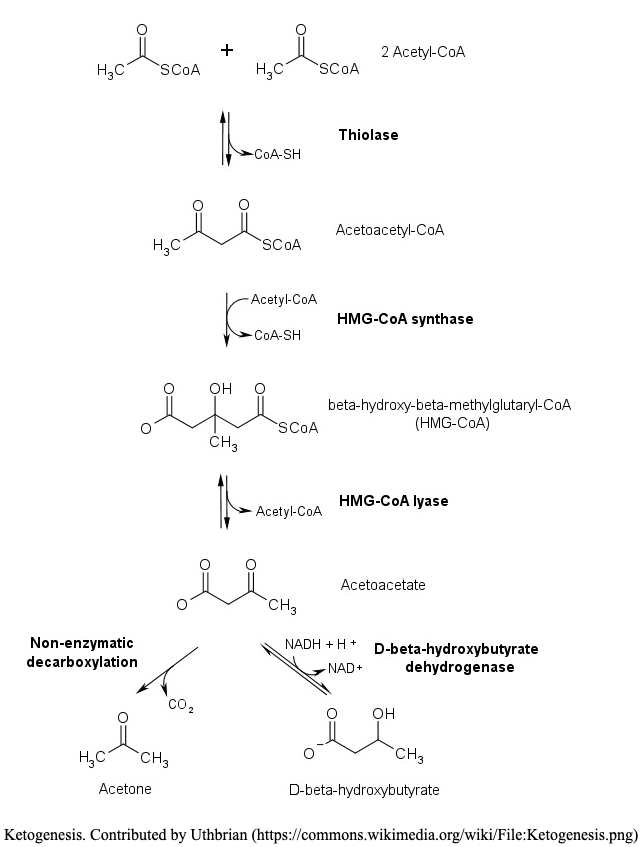
Here’s the flow diagram of ketogenesis copied from here. They in turn copied it from here. They don’t cite where they got it. But it’s a common diagram so they could have got from virtually anywhere. This is the standard diagram.
Here are the papers:
lfod14
#85
Same here, the whole adaptive glucose sparing thing always confused me, but I did notice after years of strict keto that when I did eat carbs my body completely over reacted to it, whether that’s more like a resistance or not I don’t know, but feeling like crap and then fighting consciousness isn’t fun. I do TKD now and that doesn’t happen anymore. Seems to simultaneously make sense… and not.
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#86
My question is ‘what might limit ketogenesis in long-term fat adapted individuals?’ A secondary related question is it something to be concerned about? Do we just go with the flow and accept it as a natural outcome? KCKO, etc.
The experience of greatly reduced ketones after being on keto for several years and presumably fat adapted has been noted by multiple posters here on the forum.
This is going to be a long post. So I shall break it up into pieces. This is the first piece.
Let’s first get the initial parameters out of the way. I’m talking about folks who are in long-term ketosis. These people have eaten a standard keto diet defined as ‘high fat’, ‘moderate protein’ and ‘very low/no carbs’. Pretty much Phinney and Volek’s definition of the nutrional keto diet. I’m also talking about folks who have remained consistently in nutritional ketosis for several consecutive years. By ‘consistently’ I mean specifically keeping carb intake and resultant glucose/insulin levels sufficiently low as not to interfere with continuous ketosis. This excludes anyone doing alternative keto diets such as: TKD, CKD and HPKD. Or any other iterations that intentionally/accidentally interrupt continuous ketosis whether on a regular basis or not. It’s your business not mine if you’re doing any of that, but I don’t think your experiences are relevant to answering my questions.
From Biochemistry, Ketogenesis
Mechanism
Ketogenesis occurs primarily in the mitochondria of liver cells. Fatty acids are brought into the mitochondria via carnitine palmitoyltransferase (CPT-1) and then broken down into acetyl CoA via beta-oxidation. Two acetyl-CoA molecules are converted into acetoacetyl-CoA via the enzyme thiolase; this is also known as acetyl coenzyme A acetyltransferase (ACAT). Afterward, acetoacetyl-CoA is converted to HMG-CoA via the enzyme HMG-CoA synthase. HMG-CoA lyase then converts HMG-CoA to acetoacetate. Acetoacetate can be converted to either acetone through non-enzymatic decarboxylation or to beta-hydroxybutyrate via beta-hydroxybutyrate dehydrogenase.
Acetoacetate and beta-hydroxybutyrate are the two ketone bodies used by the body for energy. Once they reach extrahepatic tissues, beta-hydroxybutyrate is converted to acetoacetate via the enzyme beta-hydroxybutyrate dehydrogenase, and acetoacetate is converted back to acetyl-CoA via the enzyme beta-ketoacyl-CoA transferase. Acetyl-CoA goes through the citric acid cycle, and after oxidative phosphorylation, produces 22 ATP per molecule. Acetone does not convert back to acetyl-CoA, so it is either excreted through urine or exhaled.
Right away, I can see multiple points of potential issues. Fatty acids are delivered to the mitochondria for processing via Carnitine Palmitoyltransferase (CPT-1). What happens if CPT-1 is not functioning normally or not produced in sufficient quantity? What if CPT-1 is ‘decoupled’ and turning fat into lost heat, as described by Bikman in his talks about BAT? What if Bikman is substantially correct that being in ketosis gives one a ‘metabolic advantage’ and that advantage is the decoupling of CPT-1 such that you’re blowing off more energy in the form of wasted heat rather than ketone synthesis? That could explain the whole thing in a single sentence. Maybe.
According to Biochemistry, Ketogenesis, after being brought into the mitochondria via CPT-1 fatty acids are then 'broken down into acetyl CoA via beta-oxidation. But that may be an outmoded description because according to The Definitive Guide:
Acetyl-CoA Formation through Fatty Acids
Acetyl-CoA formation is also said to occur via fatty acid catabolism; however, it is now understood that this acetyl-CoA is a product of carbohydrate metabolism. As acetyl-CoA can be converted into lipids and vice versa it is sometimes confused with a separate role; its true role is as a monosaccharide (glucose) metabolism catalyst.
This agrees with a comment I read from @amber in one of her blog posts about why we might have low ketones years into ketosis - the limits of acetyl-CoA due to our reduced carb consumption. Sorry I can’t cite the post, but I’ve noted it in another post, so may be able to find it and add it here.
So if we can expect lower acetyl-CoA as a result of low/no carb intake, how exactly does that impact the very first step of the process? Is some fat converted to acetyl-CoA? If so, how much? Does that amount vary individually? Or is no fat converted and gluconeogenesis has to make some glucose so it can catabolize into acetyl-CoA so the fat can catabolize further? Do we, in fact, have to synthesize some amount of glucose in order to synthesize some amount of acetyl-CoA to burn fat?
We’re not even down to:
- Two acetyl-CoA molecules are converted into acetoacetyl-CoA via the enzyme thiolase. What if you have a thiolase deficiency?
- Acetoacetyl-CoA is converted to HMG-CoA via the enzyme HMG-CoA synthase. What if you have a HMG-CoA synthase deficiency?
- HMG-CoA lyase then converts HMG-CoA to acetoacetate. What if…
I can see this is going down a rabbit hole real fast. More to come. 
Long term Keto and ketones
amber
(L. Amber O'Hearn)
#87
Thanks for the mention. The post you want is this one: Keto-adapted but no (low) ketones? Part II
I have just a couple of comments. First, the uncoupling idea wouldn’t have to do with CPT1A. CPT1A escorts the fat into the mitochondria. If you have a problem with that, you would end up with issues with both ketogenesis and gluconeogenesis. I described this case in the paper about the Arctic variant, which is linked to at the top of the post above. Slow CPT1A can be overcome with factors like high PUFA intake.
If it’s uncoupling, which happens in the mitochondria, this happens after fat is metabolised but before ATP is made with the proton gradient. I’m pretty sure ketogenesis would still happen here. In general, the more uncoupling, the higher the ketosis.
The enzyme deficiencies you mentioned, if you had them would mean you would never have high ketones. That is, this should be evident already before keto-adaptation, unless you’re suggesting that the deficiencies happen as a result of keto-adaptation?
As I mentioned in the article, I think the most likely explanation is simply lower fat to protein ratios in many lean keto-adapted people.
Long term Keto and ketones
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#88
Thank you for clarifying several points!
Yes, in fact I wondered if keto adaptation might cause reduction in some enzymes. Something has to change over time. My initial presumption was the diet remains essentially constant - resulting in consistent and continuous ketosis. Of course, if one is not consistently in ketosis all bets are off.
I’m currently testing your fat:protein ratio idea. For about 9 months I increased my protein intake to 150 grams and reduced fat intake to 222 grams per day. Aug 01, I changed back to my former ratio of 120 grams of protein and 240 grams of fat. Total calories remained approx the same: 2650-2700 daily. Although I generally eat within a 2400-2700 ‘caloric window’.
When I first got my Ketonix in 2019 I was eating to my prior ratios of 2:1 fat:protein grams. I was averaging 20-50 ppm acetone consistently daily, throughout the day. For whatever it’s worth - at the very least it confirmed consistent ketosis. I’m not convinced that acetone indicates much of anything other than you’re breaking down acetoacetate so must have some measurable level of ketones. I am currently blowing sub-10 ppm and usually sub-5 ppm multiple times per day. So I’m generating much less acetone. For whatever it’s worth - at the very least it confirms consistent ketosis. Just a lot less! I have to admit that I have not measured ketones for a year and a half, so I don’t really know exactly when the drop started and whether or not it corresponded to changing my fat:protein ratio about 9 months ago. I also don’t donate blood, so I have no idea of what my β-hydroxybutyrate levels are or how they vary during the day. I must have some because I’m in ketosis and still conscious.
So far my acetone still tests sub-10 ppm as before changing back my macro ratio. I am also eating a ‘coconut casein’ pudding every morning to up my exogenous MCT intake. My ‘pudding’ consists of 33.4 grams of casein and 25 grams each of coconut oil and MCT oil.
Thanks again for responding.
Long term Keto and ketones
amber
(L. Amber O'Hearn)
#89
Ah. Very interesting!
I would think it would take less than a week to see a change like that. Another experiment you could do is total fasting.
The other speculation I had in that post was that increased mitochondrial number might change the redox state. But I have no idea how to test that. Haha.
I’d love to hear what else you learn or think of on the topic.
Long term Keto and ketones
SunnyNC
(SunnyNC)
#90
Hi Paul and other experts on this forum.
Happy new year! I wanted to follow up on this. I am not diabetic, not yet pre diabetic :).
My A1C pre Keto was around 5.5. After 3 months Keto, it dropped to 5.2. Nice! all other numbers were fine. LDL was higher than my previous reading but HDL was superb, TG was the lowest I have seen. Total cholesterol was low just enough to be considered normal".
Since I like seeing data and tracking my numbers, I check my BG and ketone every morning using keto mojo blood meter. my fasting BG started creeping up slowly. So I started wearing a CGM to get a better picture. Luckily my doctor prescribed Libre 2 and its partly covered my insurance. Per my CGM, my fasting BG is slowly creeping up over the weeks and months. My carb count is around the same ball park, if anything I have reduced carb further by cutting down on berries and eating less veggies. I am in ketosis most of the time I check after I wake up. I do IF anywhere from 16-20 hrs every day. Post prandial BG is actually very good. It just goes up 5-15 points and goes back to baseline soon. The issue is my baseline has become very high. Per my CGM, my average BG was 96 3 months ago. Now its up to 105 which translates to 5.6-5.7 prediabetic A1C. I dont care if this is due to glucose sparing or low insulin, it is still high fasting BG and I am fasting most of the day. It will still cause RBC glycation. RBC does not know if my high BG is due to glucose sparing or from consuming lot of sugar and being IR as a result, to put it in a simple way. Maybe my glucogon is getting out of whack, but per my research that happens due to hepatic IR, which is in turn caused by chronic high insulin caused by high BG. I have scoured through pubmed etc and they all say pseudo IR, adaptive glucose sparing is OK and does not cause T2D. I dont find that to be true based on my numbers are heading.
I tried eating for a longer window (12:12, 14:16) couple of days but it was still the same.
Any further explanation will be much appreciated. I have not seen anywhere that papers that actually talks about physiological IR in the light of A1C going up. I am thinking of quitting keto and go on a low carb/paleo unless I see convincing explanation on why elevated fasting BG is ok on Keto. I would hate to stop keto as I it really has simplified life, I feel great, never hungry, go on long runs and not get hungry etc. I should also add. I work out regularly, very athletic and have 15-20% body fat, I am not doing keto to lose weight or any other particular reason. My entire family is plagued with diabetes and I started keto as a preventative diet. Sorry for the long post. I wanted to provide as much info as possible in a desperate attempt someone can shed light on this. and oh, btw, I wrote to my doc and the response was “I advise you to add more carbohydrates and eat more frequent meals”.
Regards,
Sunny
PaulL
(You've tried everything else; why not try bacon?)
#91
What’s happening with your HbA1C? If it’s staying reasonable, then I wouldn’t be concerned. There are two factors probably at work. One would be adaptative glucose-sparing (also known as “physiological insulin resistance”), and the other is known as the “dawn phenomenon.” The former is a general rise in serum glucose, resulting from the skeletal muscles’ preference for metabolising fatty acids, so that the glucose produced by the liver can be saved for those cells and organs that need it. (The muscles also prefer not to use ketones, either, once they are fat-adapted.)
Dawn phenomenon is a rise in serum glucose prompted by elevated cortisol, which is an evolutionary adaptation that allows us to wake ready to fight off cave bears and sabre-toothed tigers, if necessary. So people generally find their serum glucose at its highest point around the time they wake, and then it gradually drops over the course of the day.
Another thought to bear in mind is a remark by Dr. Paul Mason, an Australian sports physician who has joined the keto bandwagon, where he said in a recent presentation that his concern is not so much what the absolute level of the glucose is, but whether it stays in a reasonably narrow range, avoiding sharp spikes. He says that if the glucose is generally high, but with no spikes, that’s better than a generally low reading with high spikes.
robintemplin
(Robin)
#92
That’s interesting… I think the same thing might apply to weight. I believe my yo-yo dieting, extreme feast or extreme famine over the years was every bit as damaging to my overall health, if not more so, than just being consistently obese. I’m sure there are arguments to prove me wrong, but it sure feels true to me.
Jamesbrawn007
#93
Your situation sounds like the one described by Shawn Baker. However, that said, Kevin Stock had a very different experience on carnivore where his fasting BG was under 3mmol.
Personally, I would experiment with time restricted eating for a week or two where you stop eating earlier in the day giving yourself a good fasting period before rising. I would be interested to hear about your CGM results on such a protocol.
ctviggen
(Bob M)
#94
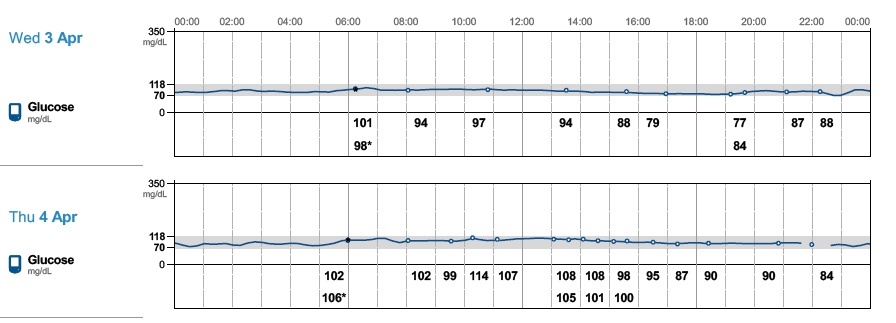
Exactly what blood sugar value are you looking at? Here’s one week’s of my data from my US Free Style Libre:

Some notes:
- I found the US FS Libre tended to read higher initially then go lower over time. My Swedish model did not do that.
- Exercise for me causes my blood sugar to go up. I think I was exercising Saturday, Tuesday and Thursday of this week (though I could be wrong). Those days have higher blood sugar readings.
- The FS Libre might not be exactly correct. You might want to check with pin-pricks or official readings.
- Does yours estimate HbA1c? If so what is it?
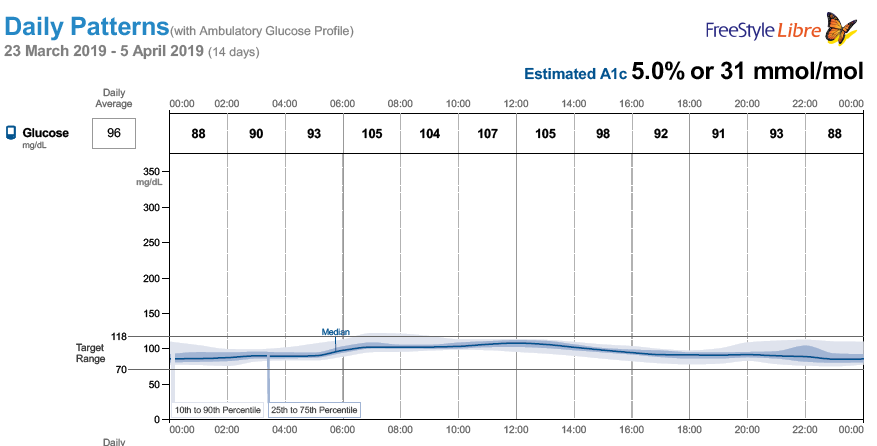
If you look at this, it starts out really high:
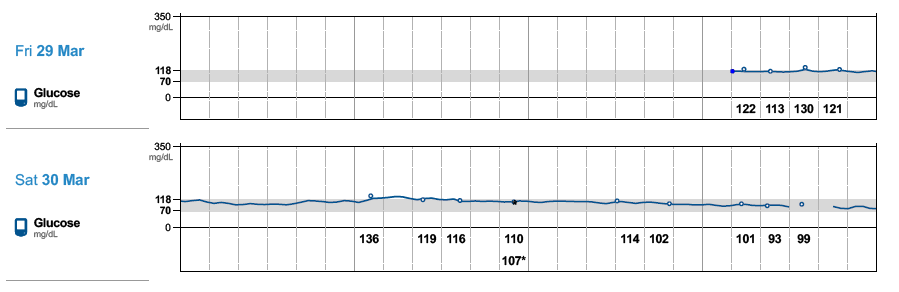
Towards the end, it read much more reasonably:
{kind=link}
My Swedish ones never had this problem.
Also, I bought a year’s supply of Swedish sensors. Of those, only a few did not last 14 days. For the US, I had none or very few last the 14 days. Not sure why.
SunnyNC
(SunnyNC)
#95
Thanks for your response, Paul. Based on my CGM data, my current A1C will be 5.7 (prediabetic). I have been spot checking GCM with ketomojo and the CGM BG reading are OK, just a few points +/-. Even exact same a few times. So I have no concerns with CGM data. While I really appreciate your response , it is does not answer my real and only question/concern - why is higher fasting BG ok, when Hb can still get glycated and cause damage? I understand this is physiologic IR and is easily reversible but that still does NOT explain how having glycated hemoglobin majority of the day is OK. The only forums I have seen it is not OK are those that are against keto.I follow low carb down under on youtube and very well familiar with Dr. Paul Mason. I have watched pretty much every video on that channel, low carb USA, and follow many Keto experts on you tube and blogs. Lately I have resorted to reading latest pubmed papers but nobody, NOBODY in the pro-keto community has answered how it is somehow magically OK to have higher fasting BG when long term fat adapted while the very same higher levels on BG can and will cause glycation regardless of presence of insulin or not. The canned response I see is high fasting BF is ok when insulin in low, get HOMA-IR test. But my question is not about IR, I know I will be very insulin sensitive if stopped keto for a few days. My only question is why is higher fasting BG ok when we know chronic high BG is the cause of many health issues. As far as I know, sugars glycate blood, insulin present or not. I also should add, when I do a water fast for 36-48 hours my fasting BG is OK (except dawn, but that drops and normalizes afternoon). So it seems like my liver is dumping excess sugar via gluconeogenesis (GNG) when I eat keto diet. I eat around 100-120g proteins well within the recommended range for my body composition and activity level. My next experiment will be to do a low protein keto for a couple of days {some call it fat fasting/ avocado diet  } and see if there are any positive changes. I am starting to believe GNG is very real in my case. Every expert out there says GNG is not something be concerned about it. Another alternative will be to try low dose metformin to reduce liver dumping sugars but its by prescription-only in US. The direction my A1C is headed, I might be able to get a prescription, lol! I just don’t like the idea of experimenting with my body but doing things for a week to test might be ok, I guess. Just laying out as much info as possible hoping others can share their view and experience with this situation.
} and see if there are any positive changes. I am starting to believe GNG is very real in my case. Every expert out there says GNG is not something be concerned about it. Another alternative will be to try low dose metformin to reduce liver dumping sugars but its by prescription-only in US. The direction my A1C is headed, I might be able to get a prescription, lol! I just don’t like the idea of experimenting with my body but doing things for a week to test might be ok, I guess. Just laying out as much info as possible hoping others can share their view and experience with this situation.
thanks for reading!
SunnyNC
(SunnyNC)
#96
I am already following a time restricted eating. I have set my goal 18-6 (18hrs fasting, 6 hours eating window) but on at least 2-3 day a week, it ends up being 20-2 as I am not hungry or too busy, and couple times a week 16:8. It averages out to 18:16. I have rarely eaten before 16 hour fasting window in the past year. I tend to stop eating around 8 PM. It is difficult for me to start eating window in the morning and end earlier. I tried that and did not like it. If there is evidence this will reduce fasting BG,I am more than willing to try again but I am pretty sure it wont help. I say this because I walk 30 minutes after my last meal and also play VR games after dinner, so I am still burning off a lot of calories post dinner. My BG actually is falling late evenings and starts raising during the early hours (dawn effect) and stays there all day long.