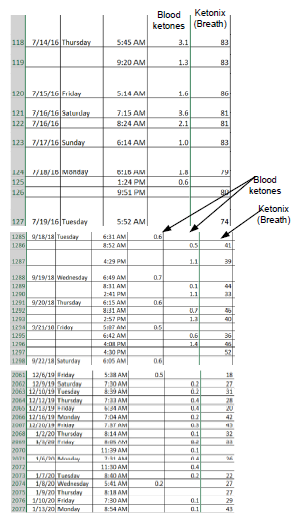
So I’ve been on this WOE for 3-years now. I wanted to know if having low ketone levels is a sign of the body being keto adapted or fat adapted. I suspect that the body will produce less ketones when the body becomes more efficient at using ketones or accessing fat stores as energy. I haven’t given a chance to buy myself a ketone meter in the 3-years of doing this diet. I’ve switched on with Carnivore style diet as well. But thing is how my fasting glucose is at its most optimal range that anyone can ever ask even during dawn phenomenon. Unless my glucose readings are inaccurate… but post exercise my blood sugar stays normal too. You may think that a low blood sugar reading around 60-70mg/dl is outrageously dangerous and have seen it dip as low in the 45’s when prolonging my fast for over 24 hours with no sudden side effects.
So if someone has low ketone levels, been doing keto for over a year long, is it to be assumed this person is fat adapted or keto adapted meaning his or her body uses fat stores, nutritional fats, and ketones as energy?