
I had my fasting insulin tested recently and it was in a very good range, but had never had it tested before. That said, last Friday I went out for my anniversary and had a rich dessert and ended up being 2.8 pounds heavier by Sunday morning. Sure sounds like my insulin kicked in big time. It took me until today to lose that that 2.8 pounds. I even did a 20 hour IF on Monday. So I am convinced that if I didn’t continue to do very low carb, I would gain rapidly again. Does that mean that I still have problems metabolically? I guess. I was never diabetic or prediabetic so I can’t comment meaningfully in that way.
Has Anyone Actually Been Tested for Insulin Resistance?
carolT
#22
The same water that goes away in the first few days of keto will come back as your liver stores glycogen again.
I doubt many people had thorough insulin testing before and after keto unless they happened to have a very good doctor. I know Peter Attia basically quit keto and went back to healthy carbs after he reversed his IR. There’s probably more anecdotal stories or clinical examples out there.
Jennibc
(Jennibc)
#23
Yes, but why did it take 6 days. Interesting is that I only gained 1.8 the first morning after and even though I went right back on plan, another pound showed up. My guess is the 1.8 was water and the 1 was actual fat based on how long it took to take off. I mean I could be wrong, but that’s my hunch.
Alecmcq
(Alec)
#25
Bunny
This is really interesting. I have always been sceptical about measuring IR, as I’ve never seen a decent test that was in any way stable, per the discussion above.
But if we use BG 2hrs after a meal as a proxy marker, and measure it after a variety of meals and average the results, it would provide a measure of IR.
Simple theory (please forgive if this is obvious and I am talking Janet and John language here): if IR is higher then the BG would be higher after a meal. If IR is lower, then insulin would work more quickly after a meal and BG would be brought down. The average BG level 2 hrs after a meal would indicate the relative level of IR. With perhaps a benchmark number being 140 or so?
My only question is whether this works if you eat a good keto meal of 1g carbs, a bit of protein and lots of lovely fat. I guess BG would go up a bit, but does it ever go up to 140?
Interesting note to self: I have NEVER measured my BG level above 6.6 mmol/l (118), but I’ve never tested after a meal… must do this.
Comments, anyone?
Jennibc
(Jennibc)
#26
No, it was at a high end steakhouse, so it was actually a modest size, but it was very rich. It was chocolate ganache mixed with hazelnuts and covered in chocolate and had a small piece of peanut brittle on top. It wasn’t like I went one of the restaurants that serves desserts in a trough.
atomicspacebunny
(Bunny)
#27
Interesting point, let’s say if you can get those pesky little GLUT4 transports to come closer to the cell surface to absorb the post meal glucose by exercising then you might not need much insulin? Like maybe chronically elevated insulin because the glucose has no where to go so the pancreas b-cells just keep pumping out more insulin trying to stuff it somewhere?
carolT
#29
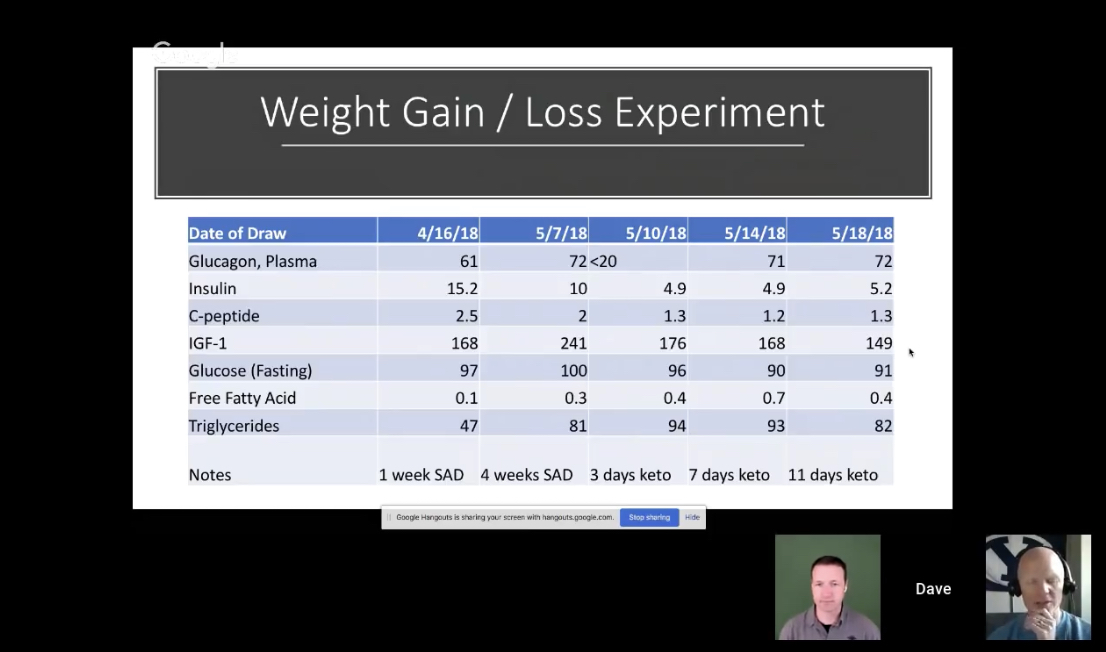
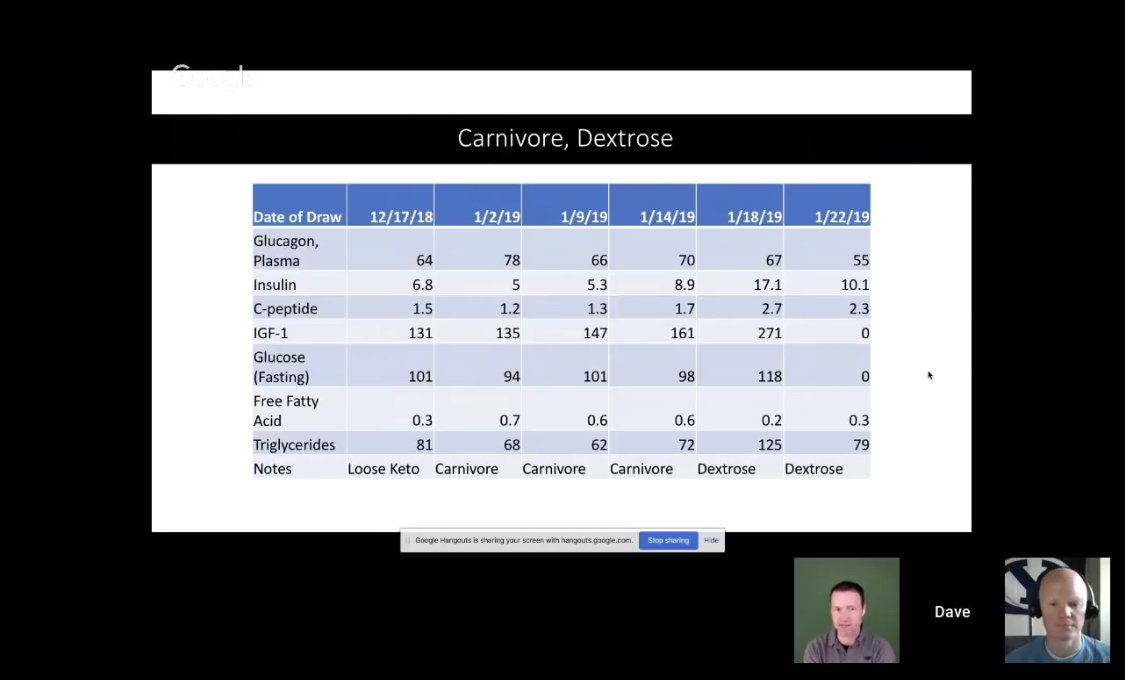
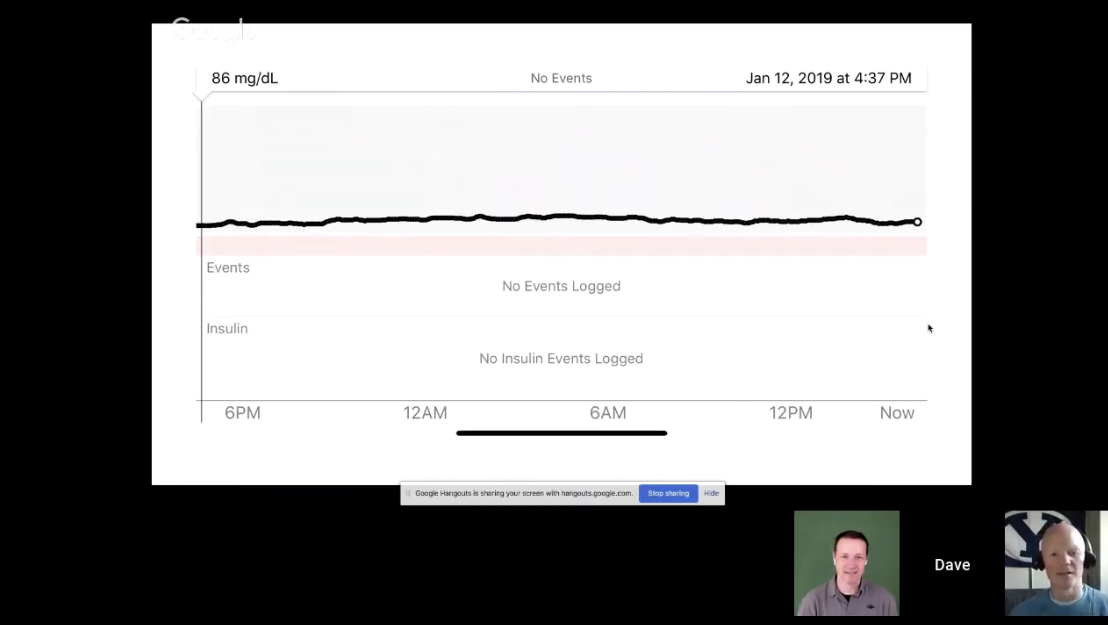
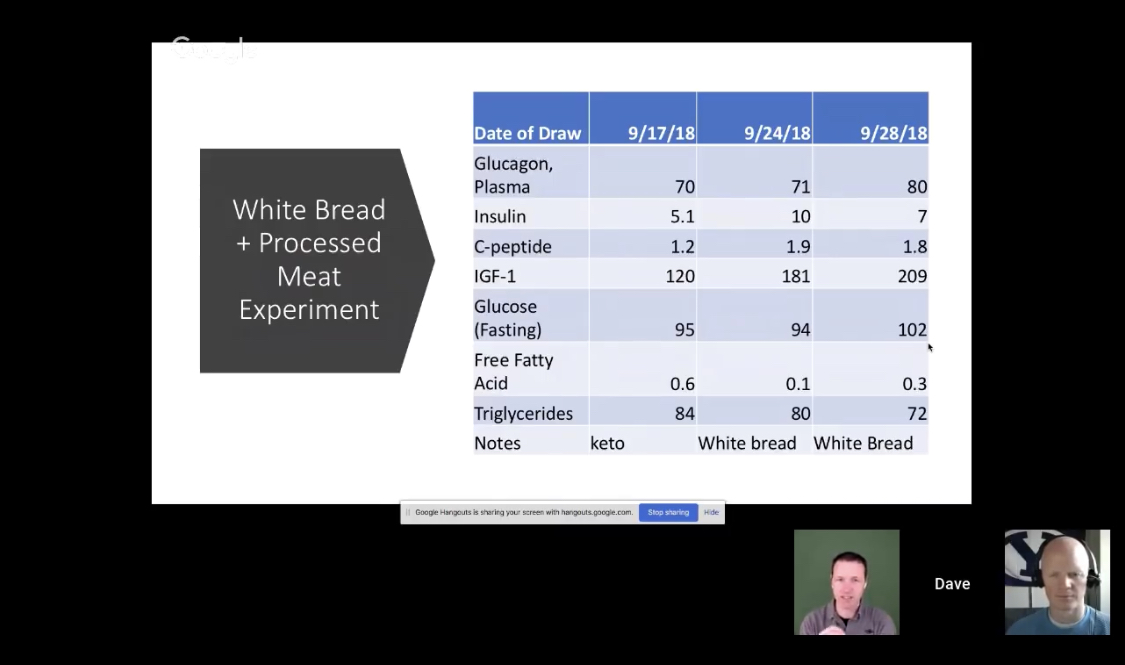
I’ve seen people (Dave Feldman) with basically flat lines on a CGM. You can’t even tell when they ate. That still doesn’t tell you how much insulin (or glucagon) they produced to keep the glucose at that level, just that they made an appropriate amount for the food they ate to be partitioned and stored in their body.
carolT
#30
Looked at another way, we could say that of the original 3650 patients who were administered the OGTT, only 15% (not 53%) were truly normal. Nearly one third of these patients had an abnormal insulin response that went undetected when looking only at glucose values.
Alecmcq
(Alec)
#31
Agreed, but wouldn’t the insulin they made to keep BG down be low? Doesn’t IR theory say that we eat, BG goes up, insulin surges to keep BG low, but if we are IR, it doesn’t work well, the BG stays high, so the pancreas pumps out another load of insulin, same thing happens again, and it keeps pumping it out until BG goes down, and this can take many many hours in those with IR. So if BG stays low, then the implication is that insulin has been minimised/kept low (which is what we want)?
carolT
#32
Simultaneous posts. 
The point where glucose does or does not remain in control is a distinct change in the progression of IR. But yes, the time glucose is elevated will get longer in time as well as higher.
I’m looking for a link to the Crofts study that has all the data…
Thanks Google.
Alecmcq
(Alec)
#33
OK, this article explains it well. So 2hr BG could be nicely low, but the pancreas has had enough time to pump out loads of insulin and we wouldn’t know. Bugger. Well that kills this theory then.
Roll on the time when we have a retail continuous insulin monitor.
carolT
#34
You can still say that if glucose is elevated there’s a problem. 
Question is, is it because even elevated insulin can’t keep it down, or insufficient insulin release because of transitory PIR on keto?
atomicspacebunny
(Bunny)
#35
Good question?
Glucagon (pancreatic and stomach lining a-cells; islands of langerhans) to glucose to insulin ratios when less fat and carbs are involved explains Dave’s flatline when protein is the primary source of nutrition which is very slowly and steadily releasing stored endogenous glucose.
Almost as if glucose is acting the same as glucagon breaking down glycogen how strange?
carolT
#37
Think of it as neligible liver glycogen, muscle glycogen is locked in muscle, glucagon-insulin regulates lipolysis (FFA). Introducing an external source of glucose doesn’t change glucagon much (baseline of individual?) but insulin cranks up to dispose of extra glucose into glycogen or adipose.
atomicspacebunny
(Bunny)
#38
”…However, even under this acute situation, the excess of glucose remains, favoring its final conversion to fat. …”
…More
Paul28023
(Paul H)
#39
Thank you all for thisI I have been down the rabbit hole for hours since reading this thread and especially since @carolT posted the video. Of course when the @atomicspacebunny gets involved my cerebral cortex whimpers. I have yet to see the video carolT posted as they say see this first and then saw another video by Dr Bikman…lol I will get there. I have really gotten alot from this post and it’s very important to me. I really agree with Dr Bikman’s point that taking insulin is like giving an addict more of what they are addicted to. It’s insulin that’s the problem…for me. Can’t wait to get off it. Just finishing this one up.
https://www.youtube.com/watch?v=uIVwrlqcyUY
Paul28023
(Paul H)
#40
One thing Dr Bikman says is that producing Ketones even if less than .5 tells us you must have low insulin. Is this something we can agree on? I am new to Dr Bikman.