
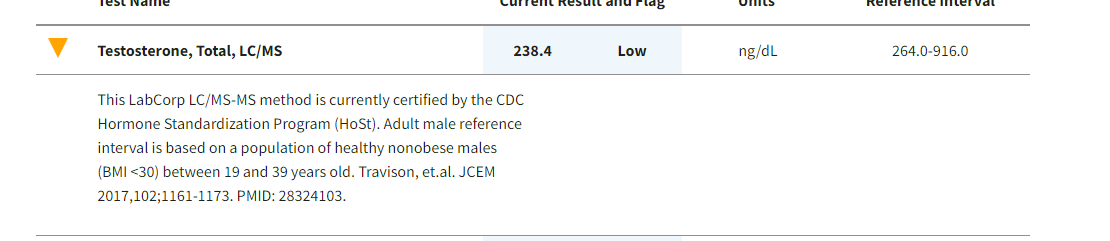
Just got my new labs
Does a healthy ketogenic diet cause irreversible insulin resistance?
fitbod
#269
SomeGuy
(Joey)
#270
Perhaps this ought to be the start of a separate thread, but I’ll reply here for now…
May I pose two (personal) questions:
1 - Do you happen to be a “healthy nonobese male (BMI<30) between 19 and 39 years old”? If not, see below.
2 - Are you suffering from some combination of these symptoms? …
- Decreased sex drive
- Decreased energy
- Depression
- Erectile dysfunction
- Infertility
- Decrease in hair growth on the face and body
- Decrease in muscle mass
- Development of breast tissue
- Osteoporosis
- Difficulty concentrating
- Hot flashes
If not, I would encourage you to stop worrying about (or even bothering to test) your testosterone levels. It’s data that’s irrelevant, non-actionable, and counterproductive to your sense of well-being.
If so, then it’s worth pursuing whether you are indeed suffering from hypogonadism, in which case testosterone replacement therapy might begin to be an option to address such symptoms.
Best wishes!
BTW, The bottom of the “Reference Range” (i.e., 95% of the subject population) for various older age groups of nonobese men in the same study which your lab report cites was found to be:
Age => Bottom of “Reference Range”
40–49 => 235
50–59 => 219
60–69=> 218
70–79=> 218
80–99=> 157
SunnyNC
(SunnyNC)
#271
I will try it next time I cycle back to Keto. Currently I switched to “slowcarb” which is pretty much carnivore-dairy+beans/lentils. Interestingly eating all the extra carbs in the form of beans and lentils has made no difference in my post meal BG. It’s pretty much the same as pre meal or even lower, similar to Keto. I definitely feel more satiated and full. My avg is trending lower than keto but I need more time to make any conclusions. I am going to do this for another week and back to keto. Will try drinking red wine then, which I love anyway and compare results.
SunnyNC
(SunnyNC)
#272
I can confirm that A1C while on keto is reliable for me. I know because it corresponds to increasing avg BG and estimated a1c based on CGM. I had posted a screenshot shot of CGM predicted avg BG and A1C. Seems pretty spot on.

amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#274
Just posted this as a new topic.
SunnyNC
(SunnyNC)
#275
Kudos for saying this. I have said this several times before but that concern somehow gets lost as the discussion turns to what causes high FBG instead of the potential harm. There are a few that do acknowledge this while believing it’s not a cause for concern. I truly appreciate and respect those comments. Tagging @Corals be as she is one of the very few that share our concern. I read in a diabetes book that the blood stickiness is much higher at 110-120 compared to 70-80. To me it’s seems like it’s common sense that it does not matter WHY the sugar is high if the end result is increasing the stickiness (via glycation). Yes less insulin in good. That’s only one part. The other part is glucose itself. Those quoting Bikman should look up his you tube video from LEVELS company. He is now saying he is not sure if high BG is ok even in fat adapted ketogenic people. He started a clinical trial to study this. Phineys Virta study - dishonest. They stopped publishing a1c results. Links in their website pertaining to high fasting BG while fasting are all now broken. This is a BIG red flag. It’s interesting the only evidence some have is evolution. My opinion is (please don’t ask me for studies, my opinion is worthless anyway), that evolution is optimized for survival of species, not longevity. I am sure some, if not all folks here are more concerned about personal long term health and longevity. Chronic stress, constant need for cortisol to induce GNG to release sugars is ok? IDK but I want to thread on the side of caution and assume that’s not good. I think cyclical KD is what I want to do for now. Till their is more research, to each their own. In the meantime, I appreciate that we can at least debate/discuss and learn what each side of this debate has to say. I am grateful I am learning new interesting thoughts/ science as a result of these forums! Cheers.
SunnyNC
(SunnyNC)
#276
Beautiful comment! Even though I have ”chosen" (maybe unwisely so) to believe the opposite, I am really fascinated by what you say. I have seen papers that claim a stable low variability is better than wild swings, for a given A1C range. They don’t however talk about - Now if the variability is low, let’s say flat line but higher in pre diabetes range, is it causing an ever so slight damage to toes and limbs? If not now, will it add up over the decades? Slow cooker vs pressure cooker, it’s a matter of time, end result my beef chilli is cooked  and it turns out I could have prevented this by keeping that line lower? Let’s say a very healthy Mediterranean style diet. We have all seen the blue zones longivity argument I am sure. My partners granddad lived to 95 perfectly healthy till the last couple months when he stopped eating when he felt his time had come. He ate meats, grains, legumes and fats every meal. Maybe he was blessed with fantastic genetics. Once again highly anecdotal and a worthless N=1 example but I think that now wants to make me want to be open minded and look into both sides more and very carefully. If someone is diabetic, I don’t have a pinch of doubt keto is the way to go. Some one that is NOT diabetic or epliptic? IDK anymore. I have shared this, perhaps useless, anecdote earlier in this thread- My partner is vegan, but eats fish couple times a month (vegan-pescatarian diet). High carb diet obviously. His TG, LDL, HDL are fantastic. His last A1C was 4.5. He is even in ketosis after over night fasting and skipping breakfast, I made him check once out of curiosity. . My numbers are all good, except the typical high LDL that us Keto folks tend to have. I did NMR which came back excellent. So not worried about LDL anymore. But my darn A1C crept up to 5.7, prediabetes. So why should I blindly assume (for myself only) that Keto is better ( despite becoming pre diabetic ) than, let’s say, healthy pescatarian, unless I have health conditions and allergies, which I currently don’t have any? I am obviously biased towards Keto because of it’s otherwise proven benefits, which I have experienced . So I hope keto is indeed the best for longivity as well! Since there is no research, I welcome any reasonable anecdotal experience. Tagging @Corals, @JustMo
and it turns out I could have prevented this by keeping that line lower? Let’s say a very healthy Mediterranean style diet. We have all seen the blue zones longivity argument I am sure. My partners granddad lived to 95 perfectly healthy till the last couple months when he stopped eating when he felt his time had come. He ate meats, grains, legumes and fats every meal. Maybe he was blessed with fantastic genetics. Once again highly anecdotal and a worthless N=1 example but I think that now wants to make me want to be open minded and look into both sides more and very carefully. If someone is diabetic, I don’t have a pinch of doubt keto is the way to go. Some one that is NOT diabetic or epliptic? IDK anymore. I have shared this, perhaps useless, anecdote earlier in this thread- My partner is vegan, but eats fish couple times a month (vegan-pescatarian diet). High carb diet obviously. His TG, LDL, HDL are fantastic. His last A1C was 4.5. He is even in ketosis after over night fasting and skipping breakfast, I made him check once out of curiosity. . My numbers are all good, except the typical high LDL that us Keto folks tend to have. I did NMR which came back excellent. So not worried about LDL anymore. But my darn A1C crept up to 5.7, prediabetes. So why should I blindly assume (for myself only) that Keto is better ( despite becoming pre diabetic ) than, let’s say, healthy pescatarian, unless I have health conditions and allergies, which I currently don’t have any? I am obviously biased towards Keto because of it’s otherwise proven benefits, which I have experienced . So I hope keto is indeed the best for longivity as well! Since there is no research, I welcome any reasonable anecdotal experience. Tagging @Corals, @JustMo
SunnyNC
(SunnyNC)
#277
They might if they are calorically deficit yet somehow kept a good metabolism going by being active all day long (job that keeps them moving all the time)? I had mentioned this earlier, my partner on high carb can get into ketosis after overnight fasting. Definitely not SAD though. More of a vegan/pescatarian Mediterranean type diet. Definitely eats a couple of heavenly hunk cookies everyday, which was my GOTO treat prior to keto. I suspect he’s in calorie deficit as he walks all day long at the hospital where he works.
PaulL
(You've tried everything else; why not try bacon?)
#278
You can’t out-exercise a poor diet. Even 20 g/day of carbohydrate is more than the amount the body likes to keep in circulation, which amounts to about a U.S. teaspoon. Given that the liver makes glucose in the absence of dietary glucose, carbohydrate is actually not necessary in the diet at all. There are no known carbohydrate deficiency diseases, whereas the consequences of failing to ingest the necessary quantity of essential amino acids and essential fatty acids are well known.
SunnyNC
(SunnyNC)
#279
Great points, once again Joey. I also wonder, at what point the benefit tips, ie some fluctuation but with lower averages is desirable over low variability but higher average… someone thats always between 135-140 cannot be better than someone that fluctuates from 70 to 140 but stays below 90 most of the time?? Most of the blood glucose studies are on diabetics and not on healthy individual due to the way funding is obtained. So I don’t think we’ll have any answers anytime soon. I hope Bikman is able to fund and conclude the levels study.
Doesn’t the burden of proof actually fall on the opposite? I mean we can all agree, for someone eating SAD, higher fasting and higher avg is generally bad. So then, is it ok on Keto, if so why? No studies means safe assumption is to lower BG till studies prove otherwise. I know all your other measurements are fine, I am just trying to, in a friendly manner, challenge why the burden of proof should be other way around like you and many others claim! If you don’t know all the pro/cons, then don’t do it (safety prioritized) Vs if you don’t know all pro/cons, do it anyway (take risk but might benefit).
Nobody here is. If you read the comments the concern is about increasing A1C
SomeGuy
(Joey)
#280
I’ve thoroughly enjoyed the exchange throughout this thread. But I’m afraid you may still be ceding the point to the Western/SAD diet “standard-of-care” trap.
Plenty of peer-reviewed research supports the conclusion that, while high HbA1c levels are strongly correlated with “known diabetics,” HbA1c is a rather poor diagnostic tool when applied to non-diabetics.
So, are we diabetic? prediabetic? struggling with metabolic syndrome?
That’s where the Oral Glucose Tolerance Test (OGTT) comes in.
Because the OGTT actually reveals the maximal glucose level before the insulin response effect kicks in. And it’s the maximal glucose level that causes the tissue damage associated with diabetes.
Someone who is alive is both inhaling and exhaling in equal volume. Based on volume/direction of airflow, on average, they’re not breathing at all. Such an average may be mathematically correct - but it’s not a good diagnostic tool.
In terms of human reproduction, there are two sexes. On average, we humans have roughly one testicle and one ovary. On a population-wide basis, these averages are accurate enough. But individual context is everything.
An HbA1c of 5.0% translates to an average glucose level of 97 mg/dL.
That 5.0% average might be the result of swings up to 200 mg/dL (diabetic), or perhaps only as high as 130 mg/dL (perfectly normal).
Context is everything. How often do they eat? How quickly is insulin released? How responsive are the insulin-sensitive tissues? How quickly does their glucose come down? And, of course, what are they eating?
The metabolic health of two individuals with identical HbA1c measures could be the difference between night and day.
When testing patients eating standard SAD who present with certain clinical signs of metabolic syndrome, the standard-of-care use of an HbA1c measure (with a reference range based on that large population who eat western SAD) for assessing risk of diabetes may be imperfect, but still somewhat useful as a first screen tool. Then an OGTT would be a logical next step to see what’s really going on.
For those who are not eating meaningful quantities of dietary glucose, I have a hard time imagining how an (assumed) 3-month average blood glucose figure can reveal much about the fasted vs post-prandial excursions of glucose and insulin in those who refrain from the SAD WOE.
Same points. Put differently? 
PaulL
(You've tried everything else; why not try bacon?)
#281
No, I don’t think so. The fact is that the bodily mechanisms regulating serum glucose evolved over two million years of a low-carbohydrate, high-fat diet (at least, according to radioisotope analysis of the bones found at archaeological digs). So it is more reasonable to assume that if someone’s glucose is higher than expected on a ketogenic diet, there is a strong possibility that’s not a problem. Note that I say possibility, because we have no data to argue either way.
Now, it is entirely possible that you have a genetic mutation that makes serum glucose over 100 deadly to you, so perhaps you are indeed right to be concerned, I don’t know. Myself, given what I have learned over the past five years on a ketogenic diet, I choose not to be so concerned—at least, given the absence of data.
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#282
I really wish we didn’t have two nearly identical topics on this subject going simultaneously. Anywhooo…
I don’t recall whether it was in this topic or the other one (and I can’t find it in either) that @PaulL said my comment on my original keto experience where I related I was not hungry until the second day of my 4-day fast that maybe I wasn’t hungry due to ketones. My observations…
I have posted numerous responses over the time I’ve been a member of the forum describing how I experienced starting keto. On ‘day 2’ I experienced what I describe as carb hunger - the incessant, demanding-to-be-fed monster reminiscent of the flesh-eating plant in the film ‘Little Shop of Horrors’. On ‘day 3’ this became what I describe as keto hunger - the company accountant announcing at the monthly board meeting that outgo exceeded income during the preceding month and the deficit was covered by the cash account.
In my case, ‘keto hunger’ replaced ‘carb hunger’ on day 3, so I conclude that during both day 1 and day 2 I was not in ketosis. Whereas on day 3 I was.
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#283
To answer the OP question unequivocally and emphatically: NO - it does NOT!
This interview with Dr Ben Bikman is about 30 minutes too long because the interviewer loves to hear the sound of her own voice. But the content pertinent to this topic starts at 46:00, which where I’ve queued the video.
PS: I found it really helpful to open the transcript and read as Bikman talks.
SomeGuy
(Joey)
#284
Good stuff. If anyone is interested, here are snippets from BYU’s bio page on Dr. Bikman:
Biography
Dr. Bikman’s research focus is to elucidate the molecular mechanisms that mediate the disruption that causes and accompanies metabolic disorders, such as obesity, type 2 diabetes, and dementia. Driven by his academic training (Ph.D. in Bioenergetics and postdoctoral fellowship with the Duke-National University of Singapore in metabolic disorders), he is currently exploring the contrasting roles of insulin and ketones as key drivers of metabolic function. He frequently publishes his research in peer-reviewed journals and presents at international science meetings.
“Much of our recent work is focused on the pathogenicity of the hormone insulin. Insulin, while necessary for healthy living, elicits significant and harmful changes in tissue metabolic function when chronically elevated. Several projects have stemmed from this work, including a focus on the varying effects of dietary macronutrients (e.g. carbohydrates vs. fats) on insulin homeostasis, the effects of insulin on brown adipose tissue (and metabolic rate), and insulin-induced brain alterations.”
Education
- Doctor of Philosophy, Bioenergetics , East Carolina University (2008)*
- Master of Science, Exercise Physiology , Brigham Young University (2005)*
- Bachelor of Science, Exercise Science , Brigham Young University (2003)*
Memberships
- American Society for Investigative Pathology (2017 - Present)*
- Mitochondrial Physiology Society (2012 - Present)*
- The Obesity Society (2012 - Present)*
- American Diabetes Association (2011 - Present)*
- American Physiological Society (2010 - Present)*
PaulL
(You've tried everything else; why not try bacon?)
#285
Since I have already seen this video linked—by you—in three other threads this morning, I am puzzled as to why you felt it necessary to link it yet one more time. It feels a bit excessive to me. Don’t you trust us to notice it the first time?
amwassil
(Michael - When reality fails to meet expectations, the problem is not reality.)
#286
Short answer: You, yes. Maybe three or four other members.
Longer answer: Lots of different folks are reading different topics. If I think a link is pertinent I will post it in those topics I think it relevant for the folks who may not be looking at the other topics where I posted it. I don’t see any problem doing so and I’ve been doing it since I joined the forum. Those who have seen it elsewhere can ignore. Or, just maybe it prompts them to recognize relevance they may not have noticed or thought about otherwise.
I should also mention that the forum software also keeps a running total of the ‘hits’ on links. So I can see how many folks have availed themselves of the info provided in the linked material.
PaulL
(You've tried everything else; why not try bacon?)
#287
So, if you are afraid that people will not pay attention the first time, what makes you feel that they will pay attention the second, third, fourth, or fifth time? At some point, you need to let the community’s response be what the community’s response will be.
PaulL
(You've tried everything else; why not try bacon?)
#289
It doesn’t matter. You make your offering to the community, and it is up to the community to do with it what it will. And if people aren’t looking at the video in the thread where you posted it originally, did it not occur to you that there might be a reason for that? This is why the software objects when you post the same link repeatedly.
Plastering the same thing all over the forums is not only unhelpful to the community, it is counter-productive for your purposes. It shouts that you don’t trust the rest of us to be capable of noticing something valuable unless you thrust it repeatedly under our noses. That kind of patronising attitude alienates people and makes them unwilling to pay attention to whatever good things you have to offer.