I think probably the most succinct and relevant thing to post would be this graph:
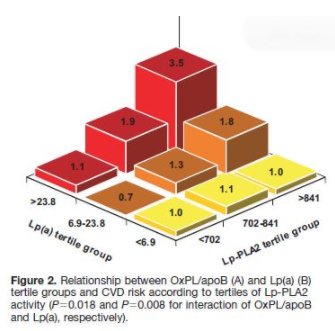
This is something that Ivor shared and it highlights that even WITH high lp(a) risk for CAD was not significantly elevated unless there was high (likely chronic) inflammation present (e.g. oxidation going on).
The more I learn about lp(a) the more I suspect that just like LDL it has different functions, some of which land it at the crime scene… but not for necessarily negative reasons (like taking on oxidized phospholipid - potentially to more rapidly clear it so damage doesnt spread).
It’s also important to note that lp(a) is partially genetic for its baseline. In theory if you have a high baseline but low oxidative stress (e.g. no smoking, low amounts of inflammatory oils, not currently sick, no refined carbs or sugar, etc - all of which are tied to higher oxstress and potentially higher lp(a) too) then it may not be an issue from what I’ve seen and what Ivor has presented as well.
Mechanistically it makes sense too. It may be there to clean up the mess, but may have other jobs too. If it’s not high because it’s cleaning up a mess, then they’re busy doing something that doesn’t have to do with heart disease (potentially).
If over all the system looks okay, it doesn’t look like theres a bunch of fires going on (inflammation, high insulin, low hdl, high triglycerides when fasting for 12-14 hours, chronically high CRP) then according to the data we currently have that doesnt necessarily imply something bad. Even in the papers I’ve gone through people sometimes just shrug and say we don’t fully understand lp(a)'s full mechanistic purpose yet. So like LDL it could turn out that it could be low or high for good or bad reasons.
We just don’t know yet, and pinning it all on one marker without context of the system imo is not wise (and Im talking about the people drumming up fear about it, here, not you).
Sorry for writing a novel here, but tl;dr even with high lp(a) risk doesn’t elevate without inflammation (chronic cause of inflammation in other words) and may be high for genetic reasons, and because it likely has multiple functions we don’t fully understand yet. Look at the system health, not a solitary marker!
Oh and as for high LDL… I wrote a post on the mechanisms of heart disease here:
You might find it useful. In short there is very good reason to believe, in my view based off of the research I’ve done so far, it is damaged LDL that is a problem in heart disease - not high LDL in itself. Give it a read and see if it gives you a different perspective 
Thanks for the tag @daveketo I swear the lp(a) post is on my to-do list 
oh and… one more thing. You mentioned trying to lower LDL to prevent lp(a) production but because the system is very good at getting the message out when it needs something if signals are sent that say “I need lp(a)” or “I need LDL” they’ll be made. Period.
The point isnt to wipe them out, at least to me, it’s to understand why theyre being made and determine if it’s a sign that some sort of damage is going on. (which is gained by looking at all your markers together as a whole).
I hope that helps!

